Abstract: WPA Congress 2014: ICD-11 Symposia: Proposals and evidence for the ICD-11 classification of bodily distress disorders
January 13, 2015
Post #320 Shortlink: http://wp.me/pKrrB-43v
Edited version of the text published on 13.01.15.
Screenshot: ICD-11 Beta drafting platform, public version, 13.01.15; Chapter 07 Mental and behavioural disorders: Bodily distress disorder. Joint Linerarization for Mortality and Morbidity Statistics (JLMMS) view selected.
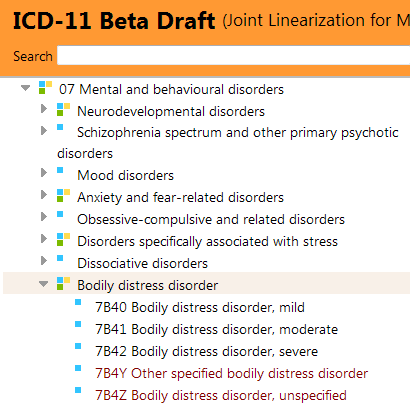
“Show availability in main linearizations” view selected. Hover text for categories designated with three coloured key reads: “In Mortality and Morbidity, Primary Care High Resource, Primary Care Low Resource.” Hover text for categories designated with single blue key reads: “In Mortality and Morbidity.”
Two working groups, two sets of recommendations
The Expert Working Group on Somatic Distress and Dissociative Disorders (S3DWG) is one of two working groups advising the Mental Health Topic Advisory Group (TAG) on the potential revision of the ICD-10 Somatoform disorders categories for ICD-11.
The other group tasked with making recommendations on the revision of the Somatoform disorders is the Primary Care Consultation Group (PCCG), led by Prof Sir David Goldberg [1].
The S3DWG’s disorder construct is the construct that has been entered into the ICD-11 Beta drafting platform since 2012 [2].
Perversely, the S3DWG is proposing to call its disorder construct, “Bodily distress disorder” (BDD) – a term already being used outside ICD Revision, interchangeably, with Bodily Distress Syndrome (BDS), which is conceptually different.
To further muddy the waters, the PCCG has proposed calling its construct (which in 2012 had drawn heavily on the Fink et al BDS concept but with some DSM-5 SSD-like psychobehavioural features tacked on), “Bodily stress syndrome” (BSS).
So four very similar terms in play:
Bodily distress disorder (S3DWG, the construct entered into the Beta draft)
Body distress disorders (PCCG primary care disorder group heading*)
Bodily stress syndrome (PCCG disorder category sitting under Body distress disorders*)
Bodily Distress Syndrome (Fink et al, 2010)
*As proposals of the Primary Care Consultation Group had stood in mid 2012 [1].
The co-chair of the Mental Health TAG agrees that the S3DWG’s BDD and Fink et al’s (2010) BDS construct [3] are conceptually different; that there is potential for confusion between the two constructs and he will be discussing the issue of BDD terminology with the working group.
I shall be reporting on some recently proposed revisions to the definition text for BDD and its three Severities in my next post.
ICD-11 Symposia, XVI World Congress of Psychiatry, Madrid 2014
The have been no progress reports from either the S3DWG or the PCCG since emerging proposals for both working groups were published in 2012.
In September, Professor Oye Gureje, who chairs the ICD-11 Expert Working Group on Somatic Distress and Dissociative Disorders, presented on “Proposals and evidence for the ICD-11 classification of Bodily Distress Disorders” as part of series of symposia on the development of the ICD-11 chapter for mental and behavioural disorders, at the World Psychiatric Association XVI World Congress, in Madrid.
In the absence of progress reports, I have requested that WHO/WPA make a transcript, slides or summary of this presentation publicly available.
In the meantime, the Abstracts for these ICD-11 symposia presentations can be found here:
http://www.tilesa.es/wpamadrid2014/abstracts/volume8/files/assets/basic-html/page352.html
also: http://www.tilesa.es/wpamadrid2014/abstracts/volume8/index.html#/352/zoomed
XVI World Congress of Psychiatry. Madrid 2014
Volume 2. Abstracts Regular Symposia[…]
http://www.tilesa.es/wpamadrid2014/abstracts/volume8/files/assets/basic-html/page354.html
Session: Regular Symposium SPEAKER 3 Code SY469
Title: Proposals and evidence for the ICD-11 classification of bodily distress disorders
Speaker O. Gureje University of Ibadan, Ibadan, Nigeria Abstract Objectives:
The disorder categories currently classified in the group of Somatoform Disorders in ICD-10 have been the subject of controversy relating to their names, utility, reliability and acceptability.
The ongoing development of ICD-11 presents an opportunity to revise these categories so as to enhance their utility and overall acceptability.
Methods: The WHO ICD-11 Working Group on Somatic Distress and Dissociative Disorders has conducted a comprehensive review of the current status of Somatoform Disorders, drawing on literature from across the world and considered within diverse clinical experiences of experts who were consulted for the revision exercise. Proposals for DSM-5 and their suitability for global application were also considered.
Results: Important areas for improving the utility and reliability of disorders grouped under Somatoform Disorders were identified. These areas encompass name, content, structure and clarity of the phenomenology. A simplified category of Bodily Distress Disorder with an improved set of guidelines for making the diagnosis has been proposed to replace current Somatoform Disorders categories.
Bodily Distress Disorder may be described as Mild, Moderate, or Severe based on the extent of focus on bodily symptoms and their interference with personal functioning. Bodily Distress Disorder is currently a subject of tests of its utility and reliability in internet- and clinic-based studies via the extensive network that WHO has developed.
Conclusions: Bodily Distress Disorder holds the promise of addressing the various concerns that have been expressed in regard to the utility and applicability of categories currently classified under Somatoform Disorders. The overarching goal of the new category is to enhance the clinical care of patients presenting with these common and disabling conditions. Bodily Distress Disorder is currently a subject of tests of its utility and reliability in internet- and clinic-based studies, including in primary care settings, via the extensive network that WHO has developed.
References Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. International Review of Psychiatry 2012; 24:556-567
Further reading:
1 Lam TP, Goldberg DP, Dowell AC, Fortes S, Mbatia JK, Minhas FA, Klinkman MS: Proposed new diagnoses of anxious depression and bodily stress syndrome in ICD-11-PHC: an international focus group study. Family Practice (2013) 30 (1): 76-87. Full free text: http://fampra.oxfordjournals.org/content/30/1/76.long
2 Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry 2012;24:556-67. [Abstract: PMID: 23244611]
3 Fink P, Schröder A. One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders. J Psychosom Res. 2010 May; 68(5):415-26. [Abstract: PMID: 20403500].
Caveats: The ICD-11 Beta drafting platform is not a static document: it is a work in progress, subject to daily edits and revisions, to field test evaluation and to approval by ICD Revision Steering Group and WHO classification experts. Not all new proposals may survive ICD-11 field testing. Chapter numbering, codes and sorting codes currently assigned to ICD categories may change as chapters and parent/child hierarchies are reorganized. The public version of the Beta draft is incomplete; not all “Content Model” parameters display or are populated; the draft may contain errors and category omissions.




