November 6, 2013
by admindxrw
Update to ICD-11 Beta draft at February 3, 2014:
Since my update on January 3, in the ICD-11 Beta draft, Hypochondriasis (illness anxiety disorder) has since been reverted to Hypochondriasis with illness anxiety disorder listed, instead, as an Inclusion term to Hypochondriasis.
Hypochondriasis was subsequently assigned to three parents:
Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere; Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders;
At February 3, Hypochondriasis has been removed from parent Bodily distress disorders and is currently assigned dual parentage under:
Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders
Foundation View:
hppt://apps.who.int/classifications/icd11/browse/f/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
Joint Linearization for Mortality and Morbidity Statistics View:
http://apps.who.int/classifications/icd11/browse/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
The Definition for Hypochondriasis currently displaying in the Beta draft appears to be the legacy Definition, unrevised from ICD-10.
Update to ICD-11 Beta draft at January 3, 2014:
Revision to ICD-11 Beta draft: In the report below, I stated:
ICD-11 public version Beta draft: Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
As the ICD-11 Beta drafting platform now stands, at January 3, 2014, the DSM-5 term “(illness anxiety disorder)” has been removed from the “Hypochondriasis (illness anxiety disorder)” disorder name and the term reverted to Hypochondriasis.
The term “illness anxiety disorder” is now displaying as listed under “Synonyms” to Hypochondriasis in the ICD-11 Beta Foundation View, and listed under “All Index Terms” in the Morbidity Linearization View.
As previously posted on November 6, 2013:
In the previous four posts, I have documented the September 18-19, 2013 meeting of the ICD-9-CM Coordination and Maintenance Committee and reported on American Psychiatric Association (APA) proposals for inserting a number of new DSM-5 terms into the forthcoming US specific ICD-10-CM.
I also set out how public and professional stakeholders can submit comment or objections on any of the proposals requested at this meeting before the November 15 deadline.
At the September meeting, Darrel Regier, MD, APA Director of Research, presented six diagnoses that are new to DSM-5 for inclusion within ICD-10-CM, with proposals for assigning unique new codes to these disorders for October 2015 [1].
Some of the DSM-5 disorders, below, presented for consideration for inclusion in ICD-10-CM are already entered into the ICD-11 Beta drafting platform and in some cases, entered into the draft over a year or more ago.*
*Caveat: The ICD-11 Beta draft is not approved by WHO or WHA. The Beta draft is a work in progress over the next two to three years. The Beta draft is updated on a daily basis: parent terms, category terms, sorting codes and descriptive content are subject to change as chapter reorganization progresses. This post reflects the Beta draft as it stood on November 6, 2013. ICD-11 Beta Draft Caveats
Binge eating disorder (BED)
(Rationale: Page 32, Diagnosis Agenda: Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Binge eating disorder (BED) as an inclusion term to F50.8 Other eating disorders.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created for F50.81 Binge eating disorder.
ICD-11 public version Beta draft: Binge eating disorder currently proposed to be coded under Feeding and eating disorders and assigned a unique ICD-11 code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Binge eating disorder.
——————————
Gender Identity Disorder in Adolescence and Adulthood
(Rationale: Page 34, Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: that ICD-10-CM change the code for Gender identity disorder in adolescents and adulthood to F64.0 and that “gender dysphoria in adolescents and adults” is added as an inclusion term for this entry.
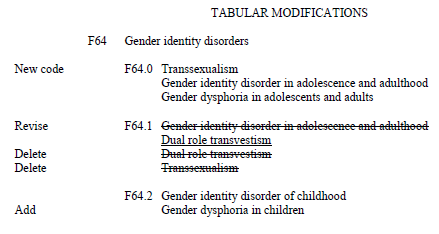
Source: September 2013 Diagnosis Agenda, Page 34
[See Page 34 of Diagnosis Agenda for discussion of proposed coding changes.]
——————————
Disruptive mood dysregulation disorder (DMDD)
(Rationale: Page 35, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Disruptive mood dysregulation disorder (DMDD) as an inclusion term under F34.8: Other persistent mood [affective] disorders.
Proposal for ICD-10-CM for October 1, 2015: that unique new codes are created at F34.81 Disruptive mood dysregulation disorder and F34.89 Other specified persistent mood disorders.
ICD-11 public version Beta draft: Disruptive mood dysregulation disorder (DMDD) is not currently listed.
——————————
Social (Pragmatic) Communication Disorder
(Rationale: Page 37, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Social (Pragmatic) Communication Disorder as an inclusion term under F80.89 Other developmental disorders of speech and language.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F80.82 Social pragmatic communication disorder.
Excludes1: Asperger’s syndrome (F84.5)
Autistic disorder (F84.0)
ICD-11 public version Beta draft: Social (Pragmatic) Communication Disorder is not currently listed.
——————————
Hoarding disorder
(Rationale: Page 39, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Hoarding disorder as an inclusion term to F42 Obsessive Compulsive Disorder.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.2 for Obsessive Compulsive Disorder and F42.3 for Hoarding Disorder in future revisions. (Ms. Pickett stated that new code proposal starting at F42.2 is due to F42.0 and F42.1 deactivation by WHO.)
F42 Obsessive compulsive disorder
New code F42.2 Mixed obsessional thoughts and acts
New code F42.3 Hoarding disorder
New code F42.8 Other obsessive compulsive disorder
New code F42.9 Obsessive-compulsive disorder, unspecified
ICD-11 public version Beta draft: Hoarding disorder currently proposed to be coded under parent Obsessive-compulsive and related disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Hoarding disorder.
——————————
Excoriation (skin picking) disorder
(APA Rationale: Page 41, Diagnosis Agenda, Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Excoriation (skin-picking) disorder as an inclusion term to L98.1 Factitial dermatitis (Dermatology section).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.4 Excoriation (skin-picking) disorder.
Excludes1: Factitial dermatitis (L98.1)
Other specified behavioral and emotional disorders with onset usually occurring in early childhood and adolescence (F98.8)
ICD-11 public version Beta draft: Excoriation disorder (skin-picking disorder) currently proposed to be coded under Obsessive-compulsive and related disorders under parent Body-focused repetitive behaviour disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Excoriation (skin-picking) disorder.
——————————
Premenstrual dysphoric disorder (PMDD)
(APA Rationale: Page 43, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
APA considers that placing PMDD outside the recurrent depressive disorder category is less than optimal for differentiating it from ICD-10-CM N94.3 Premenstrual Tension Syndrome, which is generally less severe than PMDD, and does not require psychiatric treatment. If an alternative code in the F32 series is possible, APA would prefer to modify the code in that section in future revisions.
Proposal for ICD-10-CM for October 1, 2014: add Premenstrual dysphoric disorder as an inclusion term to N94.3 Premenstrual tension syndrome (Chapter 15 Diseases of the genitourinary system).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created under Chapter 5 F32.8 Other depressive episodes.
New code F32.81 Premenstrual dysphoric disorder
Excludes1: premenstrual tension syndrome (N94.3)
ICD-11 public version Beta draft: Premenstrual dysphoric disorder (PMDD) currently proposed to be dual coded under Chapter 15 Diseases of the genitourinary system > Premenstrual tension syndrome and also coded under Chapter 5 Depressive disorders and assigned a unique code. A draft ICD-11 Definition has been populated for PMDD but no other ICD-11 “Content Model” descriptive parameters have been populated.
——————————
Somatic symptom disorder and Illness anxiety disorder
Source: September 2013 Diagnosis Agenda, Page 45
Somatic symptom disorder:
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
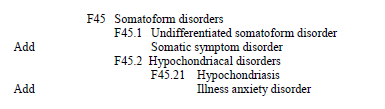
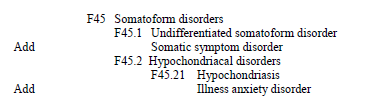
Proposal for ICD-10-CM: add Somatic symptom disorder under F45 Somatoform Disorders as inclusion term to F45.1 Undifferentiated somatoform disorder.
ICD-11 public version Beta draft: There is no Somatic symptom disorder in the ICD-11 Beta draft either as a unique new ICD-11 entity code or as an inclusion term or Synonym to an existing ICD-11 code.
For ICD-11 Core version: the current proposal for the F45 Somatoform disorders is for a proposed new construct, Bodily distress disorder, to replace a number of existing ICD-10 categories under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere. Two specifiers: Bodily distress disorder and Severe Bodily distress disorder have yet to be defined or characterized within the Beta draft and no “Content Model” parameters have yet been populated. ICD-11 plans to field test this proposed new ICD-11 construct.
The Definition for Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere currently displaying in the Beta draft appears to be the legacy Somatoform disorders Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
——————————
Illness anxiety disorder
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Illness anxiety disorder under F45 Somatoform disorders as inclusion term to F45.21 Hypochondriasis.
ICD-11 public version Beta draft: Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
The Definition for Hypochondriasis (illness anxiety disorder) currently displaying in the Beta draft appears to be the legacy Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
Submitting comments
If you have comments or objections to any of the proposals requested at the September ICD-9-CM C & M Committee meeting, the deadline for submissions is November 15, by email, to Donna Pickett: nchsicd9CM@cdc.gov
+++
References for key documents:
1. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1750103
2. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm#public_meetings
September meeting Proposals [PDF – 342 KB]
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
September meeting Summary of Diagnosis Presentations PDF file [PDF – 347 KB]:
http://www.cdc.gov/nchs/data/icd/icd_summary_sept_181913.pdf
3. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18-19, 2013 meeting materials and four YouTubes of proceedings:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/ICD-9-CM-C-and-M-Meeting-Materials-Items/2013-09-18-MeetingMaterials.html
4. September 19, 2013 Meeting Day Two: ICD-9-CM Coordination and Maintenance Committee Meeting Part 4 videocast:
http://www.youtube.com/watch?v=G-pYdKyr_NE
5. ICD-11 Beta drafting platform (public version):
http://apps.who.int/classifications/icd11/browse/f/en
 2013 All rights reserved. Current Biology,
2013 All rights reserved. Current Biology, 


Which new DSM-5 disorders proposed for inserting into ICD-10-CM are already added to the ICD-11 Beta draft?
November 6, 2013 by admindxrw
Post #280 Shortlink: http://wp.me/pKrrB-3vs
Update to ICD-11 Beta draft at February 3, 2014:
Since my update on January 3, in the ICD-11 Beta draft, Hypochondriasis (illness anxiety disorder) has since been reverted to Hypochondriasis with illness anxiety disorder listed, instead, as an Inclusion term to Hypochondriasis.
Hypochondriasis was subsequently assigned to three parents:
Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere; Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders;
At February 3, Hypochondriasis has been removed from parent Bodily distress disorders and is currently assigned dual parentage under:
Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders
Foundation View:
hppt://apps.who.int/classifications/icd11/browse/f/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
Joint Linearization for Mortality and Morbidity Statistics View:
http://apps.who.int/classifications/icd11/browse/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
The Definition for Hypochondriasis currently displaying in the Beta draft appears to be the legacy Definition, unrevised from ICD-10.
Update to ICD-11 Beta draft at January 3, 2014:
Revision to ICD-11 Beta draft: In the report below, I stated:
As the ICD-11 Beta drafting platform now stands, at January 3, 2014, the DSM-5 term “(illness anxiety disorder)” has been removed from the “Hypochondriasis (illness anxiety disorder)” disorder name and the term reverted to Hypochondriasis.
The term “illness anxiety disorder” is now displaying as listed under “Synonyms” to Hypochondriasis in the ICD-11 Beta Foundation View, and listed under “All Index Terms” in the Morbidity Linearization View.
As previously posted on November 6, 2013:
In the previous four posts, I have documented the September 18-19, 2013 meeting of the ICD-9-CM Coordination and Maintenance Committee and reported on American Psychiatric Association (APA) proposals for inserting a number of new DSM-5 terms into the forthcoming US specific ICD-10-CM.
I also set out how public and professional stakeholders can submit comment or objections on any of the proposals requested at this meeting before the November 15 deadline.
At the September meeting, Darrel Regier, MD, APA Director of Research, presented six diagnoses that are new to DSM-5 for inclusion within ICD-10-CM, with proposals for assigning unique new codes to these disorders for October 2015 [1].
Some of the DSM-5 disorders, below, presented for consideration for inclusion in ICD-10-CM are already entered into the ICD-11 Beta drafting platform and in some cases, entered into the draft over a year or more ago.*
Binge eating disorder (BED)
(Rationale: Page 32, Diagnosis Agenda: Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Binge eating disorder (BED) as an inclusion term to F50.8 Other eating disorders.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created for F50.81 Binge eating disorder.
ICD-11 public version Beta draft: Binge eating disorder currently proposed to be coded under Feeding and eating disorders and assigned a unique ICD-11 code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Binge eating disorder.
——————————
Gender Identity Disorder in Adolescence and Adulthood
(Rationale: Page 34, Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: that ICD-10-CM change the code for Gender identity disorder in adolescents and adulthood to F64.0 and that “gender dysphoria in adolescents and adults” is added as an inclusion term for this entry.
Source: September 2013 Diagnosis Agenda, Page 34
[See Page 34 of Diagnosis Agenda for discussion of proposed coding changes.]
——————————
Disruptive mood dysregulation disorder (DMDD)
(Rationale: Page 35, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Disruptive mood dysregulation disorder (DMDD) as an inclusion term under F34.8: Other persistent mood [affective] disorders.
Proposal for ICD-10-CM for October 1, 2015: that unique new codes are created at F34.81 Disruptive mood dysregulation disorder and F34.89 Other specified persistent mood disorders.
ICD-11 public version Beta draft: Disruptive mood dysregulation disorder (DMDD) is not currently listed.
——————————
Social (Pragmatic) Communication Disorder
(Rationale: Page 37, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Social (Pragmatic) Communication Disorder as an inclusion term under F80.89 Other developmental disorders of speech and language.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F80.82 Social pragmatic communication disorder.
Excludes1: Asperger’s syndrome (F84.5)
Autistic disorder (F84.0)
ICD-11 public version Beta draft: Social (Pragmatic) Communication Disorder is not currently listed.
——————————
Hoarding disorder
(Rationale: Page 39, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Hoarding disorder as an inclusion term to F42 Obsessive Compulsive Disorder.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.2 for Obsessive Compulsive Disorder and F42.3 for Hoarding Disorder in future revisions. (Ms. Pickett stated that new code proposal starting at F42.2 is due to F42.0 and F42.1 deactivation by WHO.)
F42 Obsessive compulsive disorder
New code F42.2 Mixed obsessional thoughts and acts
New code F42.3 Hoarding disorder
New code F42.8 Other obsessive compulsive disorder
New code F42.9 Obsessive-compulsive disorder, unspecified
ICD-11 public version Beta draft: Hoarding disorder currently proposed to be coded under parent Obsessive-compulsive and related disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Hoarding disorder.
——————————
Excoriation (skin picking) disorder
(APA Rationale: Page 41, Diagnosis Agenda, Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Excoriation (skin-picking) disorder as an inclusion term to L98.1 Factitial dermatitis (Dermatology section).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.4 Excoriation (skin-picking) disorder.
Excludes1: Factitial dermatitis (L98.1)
Other specified behavioral and emotional disorders with onset usually occurring in early childhood and adolescence (F98.8)
ICD-11 public version Beta draft: Excoriation disorder (skin-picking disorder) currently proposed to be coded under Obsessive-compulsive and related disorders under parent Body-focused repetitive behaviour disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Excoriation (skin-picking) disorder.
——————————
Premenstrual dysphoric disorder (PMDD)
(APA Rationale: Page 43, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
APA considers that placing PMDD outside the recurrent depressive disorder category is less than optimal for differentiating it from ICD-10-CM N94.3 Premenstrual Tension Syndrome, which is generally less severe than PMDD, and does not require psychiatric treatment. If an alternative code in the F32 series is possible, APA would prefer to modify the code in that section in future revisions.
Proposal for ICD-10-CM for October 1, 2014: add Premenstrual dysphoric disorder as an inclusion term to N94.3 Premenstrual tension syndrome (Chapter 15 Diseases of the genitourinary system).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created under Chapter 5 F32.8 Other depressive episodes.
New code F32.81 Premenstrual dysphoric disorder
Excludes1: premenstrual tension syndrome (N94.3)
ICD-11 public version Beta draft: Premenstrual dysphoric disorder (PMDD) currently proposed to be dual coded under Chapter 15 Diseases of the genitourinary system > Premenstrual tension syndrome and also coded under Chapter 5 Depressive disorders and assigned a unique code. A draft ICD-11 Definition has been populated for PMDD but no other ICD-11 “Content Model” descriptive parameters have been populated.
——————————
Somatic symptom disorder and Illness anxiety disorder
Source: September 2013 Diagnosis Agenda, Page 45
Somatic symptom disorder:
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Somatic symptom disorder under F45 Somatoform Disorders as inclusion term to F45.1 Undifferentiated somatoform disorder.
ICD-11 public version Beta draft: There is no Somatic symptom disorder in the ICD-11 Beta draft either as a unique new ICD-11 entity code or as an inclusion term or Synonym to an existing ICD-11 code.
For ICD-11 Core version: the current proposal for the F45 Somatoform disorders is for a proposed new construct, Bodily distress disorder, to replace a number of existing ICD-10 categories under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere. Two specifiers: Bodily distress disorder and Severe Bodily distress disorder have yet to be defined or characterized within the Beta draft and no “Content Model” parameters have yet been populated. ICD-11 plans to field test this proposed new ICD-11 construct.
The Definition for Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere currently displaying in the Beta draft appears to be the legacy Somatoform disorders Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
——————————
Illness anxiety disorder
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Illness anxiety disorder under F45 Somatoform disorders as inclusion term to F45.21 Hypochondriasis.
ICD-11 public version Beta draft: Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
The Definition for Hypochondriasis (illness anxiety disorder) currently displaying in the Beta draft appears to be the legacy Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
Submitting comments
If you have comments or objections to any of the proposals requested at the September ICD-9-CM C & M Committee meeting, the deadline for submissions is November 15, by email, to Donna Pickett: nchsicd9CM@cdc.gov
+++
References for key documents:
1. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1750103
2. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm#public_meetings
September meeting Proposals [PDF – 342 KB]
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
September meeting Summary of Diagnosis Presentations PDF file [PDF – 347 KB]:
http://www.cdc.gov/nchs/data/icd/icd_summary_sept_181913.pdf
3. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18-19, 2013 meeting materials and four YouTubes of proceedings:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/ICD-9-CM-C-and-M-Meeting-Materials-Items/2013-09-18-MeetingMaterials.html
4. September 19, 2013 Meeting Day Two: ICD-9-CM Coordination and Maintenance Committee Meeting Part 4 videocast:
http://www.youtube.com/watch?v=G-pYdKyr_NE
5. ICD-11 Beta drafting platform (public version):
http://apps.who.int/classifications/icd11/browse/f/en
Share this:
Filed under American Psychiatric Association (APA), CDC, CMS, Criticism of DSM-V, DSM-5, DSM-5, ICD-10-CM, ICD-10-PCS, ICD-11, Somatic Symptom Disorder, WHO (World Health Organization) Tagged with american psychiatric association, binge eating disorder, disruptive mood dysregulation disorder, dsm-5, icd-10-cm, institute of psychiatry, NCHS, premenstrual dysphoric disorder, public comment, somatic symptom disorder