1. Next release of the ICD-11 MMS (the blue “Version for preparing implementation” platform)
It was anticipated that the ICD-11 Blue platform would continue to be updated annually to incorporate all the changes approved and implemented in the Orange Maintenance platform since the last update was released.
There has been no new release of the Blue platform since April 2019.
So, for example, the exclusions for 8E49 PVFS; BME; and CFS under 6C20 Bodily distress disorder, which were approved and implemented in the Orange Maintenance platform in January, this year, don’t yet display under the exclusions list for 6C20 Bodily distress disorder in the Blue platform.
A couple of weeks ago, I contacted the WHO’s Dr John Grove to enquire when the next update of the Blue platform was anticipated to be published.
I also asked when the Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders is expected to be finalised and released.
Yesterday, I received a response from the WHO’s Dr Robert Jakob who advised that the 2020 release of the ICD-11 Blue platform will be posted in a few weeks.
2. Proposal for deprecation of the prefix “Benign” from “Benign myalgic encephalomyelitis”
In February, I submitted a new proposal for removal of the prefix “Benign” from “Benign myalgic encephalomyelitis” citing, inter alia, the precedent of the removal of the “Benign” prefix for the final update of ICD-10 (Version: 2019).
My proposal and rationale can be read here in PDF format.
There remain hundreds of proposals waiting to be reviewed in the ICD-11 Proposal Mechanism and my proposal has not yet been processed. I am hoping it will be reviewed and accepted in time for inclusion in the ICD-11 MMS 2020 release.
3. Finalisation and publication of the CDDG
The Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders has been developed by the WHO Department of Mental Health and Substance Abuse. It is the equivalent of the ICD-10 “Blue Book”.
The descriptive texts in Chapter 06: Mental, behavioural or neurodevelopmental disorders in the core version of ICD-11 are intended for use by coders and clerical workers as a basis for statistical reporting.
The CDDG provides expanded clinical descriptions, essential (required) features, boundaries with other disorders and normality, differential diagnoses, additional features, culture-related features and codes for all mental and behavioural disorders commonly encountered in clinical psychiatry and is intended for use by mental health professionals and for general clinical, educational and service use.
The draft texts for the CDDG have not been accessible to public stakeholders for review and comment, though clinicians have been able to register to review the draft and provide feedback throughout its development, via the Global Clinical Practice Network platform.
Last year, the WHO stated that the CDDG would be published “as soon as possible” after the May 2019 adoption of ICD-11 at the 72nd World Health Assembly.
I was advised, yesterday, by Dr Jakob, that the CDDG is still being amended based on feedback from the field and that the mental health team hasn’t provided a clear deadline [for its finalisation and release].
4. Publication of the ICD-11 PHC
There is no indication when the WHO expects to finalise and release the ICD-11 PHC — a clinical guideline written in simpler language to assist non-mental health specialists, especially primary care practitioners and non medically trained health workers and also intended for use in low resource settings and low- to middle-income countries, with the diagnosis and management of common mental disorders.
The ICD-11 PHC is proposed to comprise 27 mental disorders and contains no general medical diseases. Like the ICD-10 PHC (1996), this revised diagnostic and management guideline will not be mandatory for use by member states.
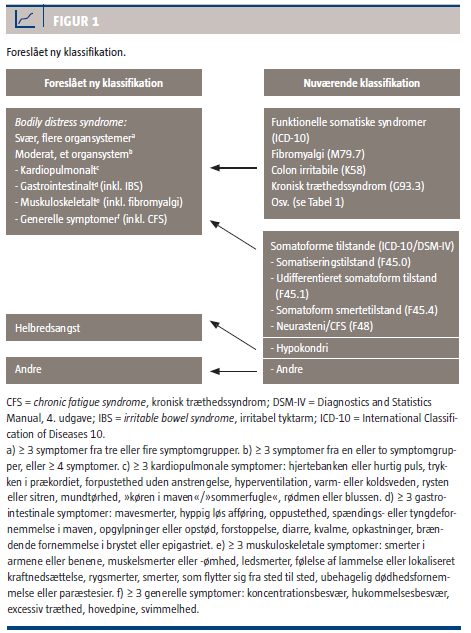
For the mandatory core ICD-11 classification, the WHO has gone forward with Bodily distress disorder (BDD), which is conceptually similar to DSM-5’s Somatic symptom disorder (SSD).
But for the ICD-11 PHC, a disorder category called “Bodily Stress Syndrome (BSS)” that has been adapted from the Fink et al (2010) Bodily distress syndrome (BDS) is proposed to be included to replace ICD-10 PHC’s F45 Unexplained somatic complaints and F48 Neurasthenia categories.
Under exclusions and differential diagnoses for BSS, certain psychiatric and general medical diagnoses have to be excluded but CFS, ME; IBS; and FM appear not to be specified as exclusions.
The ICD-11 PHC has not been developed on a publicly accessible platform and the draft texts for the 27 mental disorders proposed to be included are not available for public stakeholder review and comment.
The “Bodily Stress Syndrome (BSS)” category, its proposed text and proposed criteria need stakeholder scrutiny.
If ICD-11 PHC goes forward with its proposed BSS category, there will be all these diagnostic constructs and criteria sets in play:
Somatic symptom disorder (DSM-5; under BDD Synonyms list in the core ICD-11) Bodily distress disorder (core ICD-11; SNOMED CT) Bodily Stress Syndrome (ICD-11 PHC guideline for 27 mental disorders) Bodily distress syndrome (Fink et al 2010, operationalized in Denmark and beyond)
plus the existing ICD-10 and SNOMED CT Somatoform disorders categories and their equivalents in ICPC-2.
5. A revised version of my report “Update on classification and coding of PVFS, ME and CFS for ICD-11” (v4 August 2020) is available to download
On February 10, 2020, the WHO stated on the Proposals platform: “The ICD-11 codes are now frozen. Proposed changes to the classification that would result in a code change are not permitted.”
Changes that would not disrupt the structure of the code hierarchies, for example, additions to the Index, addition or deletion of Synonym terms or Exclusion terms, edits to category Description texts or correction of typos are permissible.
But proposals for major changes such as relocating an existing Concept Title to a different chapter (which would necessitate a code change) or moving a term under a different “primary parent” code within its current chapter could not be considered.
For further information on ICD-11 update schedules and what classes of changes are permitted see:
In May 2019, the World Health Assembly (WHO) adopted ICD-11 for implementation by member states from January 01, 2022.
In early 2019, the Australian Institute of Health and Welfare (AIHA) undertook a national consultation regarding ICD-11 to inform decisions on whether, when and how to implement ICD-11 in Australia.
The report of the AIHA was released on March 12, 2020:
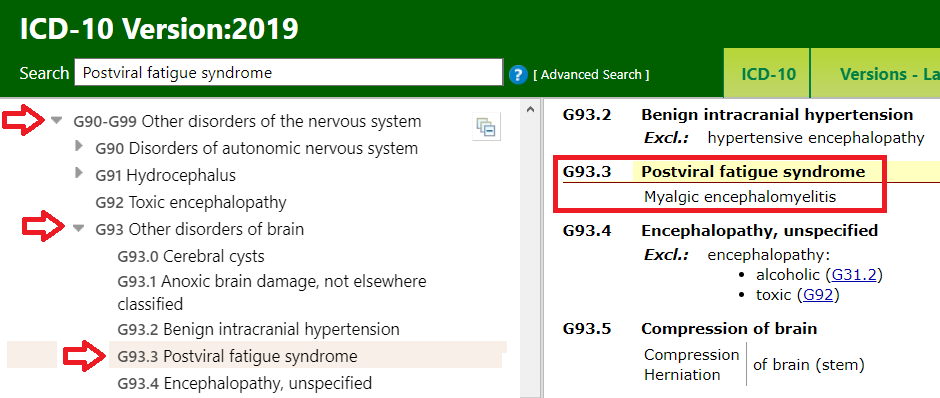
In my report for the December edition of the ME Global Chronicle, I set out how the G93.3 terms:
Postviral fatigue syndrome
Benign myalgic encephalomyelitis
Chronic fatigue syndrome
are classified in the World Health Organization’s international version of ICD-10 and how these terms have been classified for ICD-11.
I have an update on ICD-10 and it’s good news!
In January, the WHO released ICD-10 Version: 2019. With ICD-11 on the horizon, this release will be the final update for the WHO’s international version of ICD-10, apart from corrections and exceptional additions.
In March 2016, a representative from the Canadian Institute for Health Information submitted a request and supporting rationale to the ICD-10 Update and Revision Committee (URC) for removal of the prefix “Benign” from “Benign myalgic encephalomyelitis”.
This request for a change was approved by the URC in September 2016 for implementation in the next release.
For ICD-10 Version: 2019, the G93.3 Tabular List inclusion term is now Myalgic encephalomyelitis.
(The term, “Benign myalgic encephalomyelitis” has been retained as an Index term.)
Note that for ICD-10, Chronic fatigue syndrome is not included in the Tabular List but is included in Volume 3: Index, where it is coded to the G93.3 Postviral fatigue syndrome concept title term.
For ICD-11, the WHO has retained Postviral fatigue syndrome as the concept title term in Chapter 08: Diseases of the nervous system under parent: Other disorders of the nervous system. The new code for ICD-11 is: 8E49.
Benign myalgic encephalomyelitis and Chronic fatigue syndrome are both specified as inclusion terms under Postviral fatigue syndrome in ICD-11’s equivalent to the Tabular List and take the 8E49 code. A number of historical and alternative terms are retained as index terms and all 14 index terms are coded to 8E49.
This is how the G93.3 terms are classified for ICD-10 Version: 2019:
The WHO expects Member States to be using the most recent release of ICD-10. But countries will implement the ICD-10 Version: 2019 release according to their own schedules.
NHS England and ICD-10:
NHS England currently uses ICD-10 Version: 2016. I have contacted NHS Digital’s classifications lead to establish whether NHS Digital intends to implement Version: 2019 or may be considering skipping the new release in preference to implementing ICD-11, at some point in the future.
If there is no mechanism for incorporating selected changes in a new release into earlier versions, NHS England might not be able to absorb this change into the version it is using.
Will this change be absorbed automatically for ICD-11?
This revision for the final release of ICD-10 sets a precedent for the national modifications of ICD-10, for example, the U.S. ICD-10-CM and Canadian ICD-10-CA, but also for ICD-11.
Proposals submitted in March 2017 by Chapman & Dimmock, and by the IACFS/ME for removing “Benign” from “Benign myalgic encephalomyelitis” were rejected by the WHO in early 2019.
In February, I submitted a new proposal for removal of the “Benign” prefix for ICD-11 citing the URC’s 2016 decision and the implementation of that decision for the final release of ICD-10.
An edited version of this report is scheduled for publication in the March edition of the ME Global Chronicle.
For ICD-11, most of the ICD-10 F45 Somatoform disorders categories and F48.0 Neurasthenia have been replaced by a single new category called “Bodily distress disorder” (BDD).
Although this sounds like it might be very similar to Per Fink’s Bodily distress syndrome (BDS), ICD-11’s BDD is conceptually closely aligned with the DSM-5’s Somatic symptom disorder (SSD).
For ICD-11, Somatic symptom disorder is listed under Synonyms under BDD but is not coded as an inclusion term.
Both the WHO and Prof Fink have clarified that as defined for ICD-11, BDD is a conceptually different disorder construct — ICD-11’s BDD and Fink’s BDS are differently defined and characterised, have very different criteria and are inclusive of different patient sets.
For ICD-11, the BDD diagnosis requires both the presence of one or more chronic, distressing bodily symptoms (which can be “medically unexplained” or caused or exacerbated by a general medical condition) and “excessive attention” or “disproportionate or maladaptive” thoughts, feelings or behavioural responses to these symptoms. BDD can capture a percentage of patients with ME, CFS or other general medical diseases or conditions — if the clinician considers the patient also meets the disorder description for application of an additional mental disorder diagnosis of BDD.
In contrast, Fink’s BDS disorder construct requires physical “symptom patterns” or “clusters” from one or more body systems; the symptoms must be “medically unexplained” and there is no requirement for emotional or behavioural responses to meet the criteria. If the symptoms can be better explained by a general medical disease, they cannot be labelled “BDS”. But crucially, Fink’s BDS is inclusive of ME, CFS, IBS and FM and subsumes these under a single, unifying diagnosis.
The terms “bodily distress disorder” and “bodily distress syndrome” have been used synonymously since 2007. Not surprisingly, researchers, academics and practitioners are already confusing and conflating ICD-11’s new “Bodily distress disorder” with Fink’s “Bodily distress syndrome”.
Although BDD can potentially be applied to patients with chronic, distressing symptoms associated with any general medical disease or condition, patients with a diagnosis of ME or CFS (or who are waiting for a diagnosis) may be particularly vulnerable to misdiagnosis with BDD or misapplication of an additional BDD mental disorder diagnosis, as a “bolt-on” to their existing diagnosis.
However, the need for adding exclusions for PVFS, ME and CFS under ICD-11’s BDD to mitigate the risk of misdiagnosis or misapplication had not been acknowledged or accepted by the WHO.
In my report in the December edition of the ME Global Chronicle, I mentioned that the proposals submitted by Chapman & Dimmock (March 2017) and by Lily Chu MD on behalf of IACFS/ME (March 2017) for exclusions for the three 8E49 terms under 6C20 Bodily distress disorder and for exclusion of 6C20 Bodily distress disorder under the 8E49 Postviral fatigue syndrome concept title had been rejected.
In December 2019, I submitted a new proposal for exclusions for the three 8E49 terms under 6C20 Bodily distress disorder, supported by a new rationale text.
I am very pleased to inform you that in January the WHO approved and implemented my proposal.
The WHO Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD‐11 Mental, Behavioural and Neurodevelopmental Disorders:
For ICD-11, the WHO Department of Mental Health and Substance Abuse has developed the “Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD‐11 Mental, Behavioural and Neurodevelopmental Disorders” (an equivalent publication to ICD-10’s “Blue Book”).
The CDDG provides expanded clinical descriptions, essential (required) features, boundaries with other disorders and normality, differential diagnoses, additional features, culture-related features and codes for all mental and behavioural disorders commonly encountered in clinical psychiatry. This companion publication is intended for mental health professionals and for general clinical, educational and service use.
The WHO has said it planned to release the CDDG “as soon as possible” after WHA’s adoption of ICD-11. But it remains unclear whether the CDDG has been finalised or if it will be released later this year or next year.
Whilst clinicians have been able to register to review and provide feedback on the drafts, no draft texts for the CDDG have been made available for public stakeholder scrutiny and comment and I have not had access, for example, to the most recent draft for the full clinical descriptions and diagnostic guidelines for ICD-11’s Bodily distress disorder.
In 2002, I set up FreeMEuk — a Yahoo Group support and information exchange for patients with ME, CFS, and for carers, like myself. In 2007, I launched ME agenda to provide patients, carers and advocates with information, resources and commentary on the political issues affecting the lives of myalgic encephalomyelitis (ME) patients in the UK.
In January 2010, I created this site specifically to monitor and report on the development of the American Psychiatric Association’s DSM-5, the development of the World Health Organization’s ICD-11 and on other classification and terminology systems. Where appropriate, I have galvanized stakeholders to participate in review and comment exercises or co-ordinated other forms of response.
Down the years, I’ve undertaken numerous short and long-term ad hoc projects, advised others on technical matters relating to classification and terminology systems, submitted and collaborated in the submission of proposals, briefed politicians and patient organizations and kept patient forums up to date with key developments.
Today I am retiring after 17 years of advocacy work.
My sites will remain online for the foreseeable future. Over the coming months I shall be carrying out some housekeeping on this site to remove or archive older, less relevant content.
Classification and terminology systems are going to need continued monitoring; where required, input from stakeholder groups — clinicians, researchers, health practitioners and professional body allies, social workers, disability lawyers and advocacy organizations will need to be co-ordinated.
Where no process for public stakeholder input currently exists, channels of direct communication will need to be opened with the agencies responsible for the development and management of these systems and collaborative dialogues established.
WHO, for example, ostensibly gives more consideration to evidence based submissions supported by rationales, international consensus and input from clinical and professional bodies — has scant regard for patient opinion and none whatsoever for petitions or mass mailings — the latter and similar types of “action” will only undermine the careful work and discourse that I and others have fostered.
All these systems will require regular monitoring:
DSM-5:
DSM-5 published in May 2013; it has an update process which reviews formal submissions for changes to criteria, related texts, assessment measures or corrections. DSM-5 also absorbs relevant coding changes in the annual FY releases of the U.S. specific ICD-10-CM. Approved proposals are posted for a 45 day stakeholder comment period. For example, in 2015, an edit in the text for Somatic symptom disorder¹ was approved for implementation and the revised text published in the DSM-5 Update Supplement.
Member states using the WHO’s ICD-10 don’t all use the same version (or the most recent version), for example, NHS England currently mandates the use of ICD-10 Version: 2015, not Version: 2016. WHO has said that the final update to ICD-10 will be Version: 2019. This final release is understood to have been prepared but is not currently available on the ICD-10 Browser platform.
ICD-10-CM:
The U.S. uses ICD-10 for reporting mortality and developed a “clinical modification” of ICD-10 (called ICD-10-CM) for morbidity. A new release of ICD-10-CM is posted on the CDC website annually, in June.
There are two public NCHS/CDC Coordination and Maintenance Committee meetings a year through which proposals for changes to the ICD-10-CM can be submitted for discussion (in March and September) followed by a stakeholder comment period.
At the September 12, 2018 C & M Committee meeting, proposals for changes to the existing coding of R53.82 Chronic fatigue syndrome NOS; G93.3 Postviral fatigue syndrome, Benign myalgic encephalomyelitis; and a second option for addition of the SEID term were presented for consideration and public comment¹. Whilst no changes for these codes were approved for implementation in the FY 2020 ICD-10-CM release, this topic will need continued monitoring as it may be revisited at a future C & M Committee meeting for presentation of revised proposals.
1 ICD-10-CM Coordination and Maintenance Committee Meeting, September 11-12, 2018, Diagnosis Agenda Part 2
Other country specific clinical modifications of ICD-10:
Around 25 member states are also using a modification of the WHO’s ICD-10. For example: Canada (ICD-10-CA); Germany (ICD-10-GM); Australia (ICD-10-AM). Belgium, Luxembourg and Spain use ICD-10-CM; Ireland and Slovenia use ICD-10-AM.
Countries using modifications of ICD-10 have individual update cycles and varying policies around public stakeholder input and review. Some countries post their Tabular List and Index modifications in the public domain; others are available only under licence, for example, Australia’s ICD-10-AM isn’t publicly available. The coding, hierarchy and chapter location of the PVFS, BME and CFS terms differs between some of the clinical modifications, while others remain consistent with the structure of the WHO’s ICD-10.
This table from the eHealth DSI Semantic Knowledge Base project compiles information provided from a number of member states on their use of ICD (or a modification of ICD) and their plans regarding potential future implementation of ICD-11. Information has been provided by: Austria, Belgium, Croatia, Cyprus, Czech Republic, Estonia, France, Germany, Greece, Hungary, Ireland, Italy, Luxenbourg, Malta, Netherlands, Portugal, Slovenia and Spain:Current status of the use of ICD by eHDSI deploying countries (2018)
SNOMED CT:
SNOMED CT is a comprehensive clinical terminology system used in electronic patient health records. SNOMED CT maps to ICD-10 and there is a SNOMED CT to ICD-11 Mapping Project in progress.
SNOMED International has thirty-nine member countries. There is a SNOMED CT International Edition, for which two releases are issued per year (in January and July). There are a number of country specific national editions which release twice yearly updates on a staggered schedule. 12 of these national editions can be viewed on the SNOMED CT Browser platform.
SNOMED CT national editions absorb the changes in the most recent release of the International Edition but they can also include additional country specific terms. For example, the UK Edition has a unique Concept term: Medically unexplained symptoms (SCTID: 887761000000101). Prior to March 2019, the SNOMED CT Netherlands Edition had retained the term “neurasthenie” under Synonyms to Chronic fatigue syndrome, although the Concept term: Neurasthenia (SCTID: 268631001) and some associated codes had been retired from the International Edition and from all other national editions, some years ago. Following a request supported by a rationale, the term “neurasthenie” has now been removed from the Netherlands Edition.
The SNOMED CT Concept term for Chronic fatigue syndrome is SCTID 52702003 Chronic fatigue syndrome (disorder). Benign myalgic encephalomyelitis; and Myalgic encephalomyelitis are included as Synonym terms.
Following a successful submission in February 2018 for the addition of a new parent, SCTID: 52702003 Chronic fatigue syndrome (disorder) has been assigned under parent: SCTID: 118940003 Disorder of nervous system (disorder) since the July 2018 release of the SNOMED CT International Edition. This change of parent has been incorporated into the national editions.
The International Edition and the national editions of SNOMED CT will need monitoring twice yearly for changes and additions to their content.
ICD-11:
On May 25, 2019, the 72nd World Health Assembly voted unanimously to adopt the ICD-11. The earliest date from which member states can start using the ICD-11 code sets for reporting data is January 1, 2022. Countries are beginning to evaluate the new edition and develop road maps but even early implementers are anticipated to take several years to prepare their health systems for migration. There is no mandatory implementation date and countries will transition to ICD-11 at their own pace and according to their resources and requirements. For some years to come, WHO will be accepting data reported using both ICD-10 and ICD-11 code sets.
ICD-11 update and maintenance: The current release of ICD-11 (Version 04/2019) on the Blue ICD-11 MMS platform is a stable release but an update and maintenance cycle is already in place.
The various ICD-11 Topic Advisory Groups and sub working groups, the Revision Steering Group and the Joint Task Force have all been sunsetted. WHO is now advised on how to process proposals for changes to ICD-11 by the Family of International Classifications Network (WHO-FIC); the Classifications and Statistics Advisory Committee (CSAC); the Medical and Scientific Advisory Committee (MSAC); the Mortality and Morbidity Reference Groups; and the Functioning and Disability Reference Group.
Updates that impact on international reporting (the 4 and 5-digit structure of the stem codes) will be published every five years. Updates at a more detailed level can be published at annual rates. Additions to the ICD-11 index can be done on an ongoing basis. (There are currently in the region of 1200 unprocessed proposals waiting to be processed, with new proposals being submitted daily by WHO, professional bodies and other stakeholders.)
PVFS, BME, CFS: In a decision supported by the MSAC and CSAC committees, WHO rightly rejected the proposal of Dr Tarun Dua/Topic Advisory Group Neurology to delete the G93.3 legacy terms from the Diseases of the nervous system chapter and reclassify these terms in the Symptoms, signs chapter, under Symptoms, signs or clinical findings of the musculoskeletal system.
All three terms have been retained under their legacy chapter, under parent class: Other disorders of the nervous system, with 8E49 Postviral fatigue syndrome retained as the Concept Title. Benign myalgic encephalomyelitis; and chronic fatigue syndrome are both specified as Inclusion terms. Reciprocal exclusions for MG22 Fatigue were submitted for and approved.
The Proposal Mechanism platform for ICD-11 will need constant surveillance: there are currently no unprocessed proposals pending review for PVFS, BME and CFS. To date, WHO has rejected proposals for deprecation of the word “Benign” from Benign myalgic encephalomyelitis. This will need pursuing.
BDD: A proposal submitted by a third party in April 2017 for Deletion of 6C20 Bodily distress disorder has remained under review with the CSAC committee. According to WHO admins, in June 2019: “This proposal is being sent to MSAC to ensure the precedent decision on this issue still stands. Team3 WHO2019-Jun-12 – 16:40 UTC”
(In February 2019, my own recommendations for 6C20 Bodily distress disorder had been marked as rejected by a different WHO admin team, with the comment: “This proposal has been extensively discussed by WHO and its advisory committees. There is no new scientific evidence to support this proposal and it will not be further processed. Team 2 WHO2019-Feb-26 – 23:04 UTC“)
On December 02, 2019 I submitted a new proposal and rational for adding exclusions for PVFS; BME; and CFS under 6C20 Bodily distress disorder. The WHO approved and implemented my proposal on January 17, 2020.
For more information on approved and rejected proposals see: Status of ICD-11 processed proposals v5 (updated to reflect implementation of exclusions under BDD).
Clinical modifications of ICD-11:
It is understood that the WHO would prefer to limit the development of national modifications and that policies around the licensing of ICD-11 are still being formulated. Countries developing modifications of ICD-11 will need surveillance.
ICD-11 and the CDDG guideline for mental disorders:
For ICD-11, the WHO Department of Mental Health and Substance Abuse has developed the “Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD‐11 Mental, Behavioural and Neurodevelopmental Disorders” (an equivalent publication to ICD-10’s “Blue Book”).
The CDDG provides expanded clinical descriptions, essential (required) features, boundaries with other disorders and normality, differential diagnoses, additional features, culture-related features and codes for all mental and behavioural disorders commonly encountered in clinical psychiatry; it is intended for mental health professionals and for general clinical, educational and service use.
Whilst clinicians have been able to register to review and provide feedback, no draft texts for the CDDG have been made available for public stakeholder scrutiny and comment and I have not had access, for example, to the most recent draft for the clinical descriptions and diagnostic guidelines for ICD-11’s Bodily distress disorder.
ICD-11 and the ICD-11 PHC:
Also under development is the WHO’s ICD-11 PHC — a clinical guideline written in simpler language to assist non-mental health specialists, especially primary care practitioners and non medically trained health workers, and also intended for use in low resource settings and low- to middle-income countries, with the diagnosis and management of common mental disorders. It comprises 27 mental disorders and contains no other disorders or diseases. Like the ICD-10 PHC (1996), this revised diagnostic and management guideline will not be a mandatory classification for member states.
For the mandatory core ICD-11 classification, WHO is going forward with the SSD-like Bodily distress disorder (BDD).
It’s not known when this guideline is expected to be finalized and made available for download. The ICD-11 PHC has not been developed on a publicly accessible platform and draft texts are not available for public stakeholder review and comment. This non mandatory 27 mental disorder guideline needs close scrutiny.
ICPC-3:
The WONCA developed and WHO endorsed, International Classification of Primary Care (ICPC-2) is under revision for ICPC-3.
ICPC-2 is available in 34 countries; used in primary care in 27 countries and is mandatory in 6 EU countries, eg the Netherlands. The content of ICPC-3 will be linked to relevant classifications, such as ICD-10, ICD-11, ICF, ICHI, DSM-5, clinical terminologies such as SNOMED-CT, but also to previous versions of ICPC.
The draft content for ICPC-3 is not being developed on a publicly accessible platform and it’s unclear whether any form of stakeholder review will be undertaken or at what point.
Dr Marianne Rosendal (Aarhus University), who has published with Prof Per Fink, is the European representative on WONCA’s International Classification Committee and a member of the revision committee for ICPC-2, as is the U.S.’s, Dr Michael Klinkman. ICPC-2 meeting summary documents dating from 2010/2011 indicate that Dr Rosendal has discussed the potential for inclusion of a Bodily distress syndrome or similar disorder concept in the ICPC-3. Prof Per Fink is likely to be lobbying hard for its inclusion. The development of ICPC-3 will need very close monitoring.
In the World Health Organization’s ICD-10 Tabular List there are no disease or disorder descriptions, criteria or diagnostic guidelines in any chapters other than the brief description texts for disorders coded within Chapter V Mental and behavioural disorders.
The WHO describes these brief description texts as suitable for use by coders or clerical workers and to serve as a reference point for compatibility with other classifications. These brief texts are not recommended for use by mental health professionals.
Two companion publications were developed for use with ICD-10’s Chapter V which expand on these brief texts and provide clinical descriptions and diagnostic guidelines. These publications are available as license free downloads:
The ICD-10 Classification of Mental and Behavioural Disorders: Clinical descriptions and diagnostic guidelines (aka the “Blue Book”) intended for mental health professionals for general clinical, educational and service use:
The ICD-10 Diagnostic criteria for research (aka the “Green Book”) produced for research purposes and designed to be used in conjunction with the Clinical descriptions and diagnostic guidelines “Blue Book”:
A survey of nearly 5,000 psychiatrists in 44 countries sponsored by the WHO and the World Psychiatric Association found that 70% of respondents mostly used the ICD-10 classification system in their daily clinical work compared to 23% of practitioners primarily using the American Psychiatric Association’s DSM-IV [1].
ICD-11 and the CDDG
For ICD-11, the WHO Department of Mental Health and Substance Abuse has developed the “Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD‐11 Mental, Behavioural and Neurodevelopmental Disorders.”
The CDDG provides expanded clinical descriptions, essential (required) features, boundaries with other disorders and normality, differential diagnoses, additional features, culture-related features and codes for all mental and behavioural disorders commonly encountered in clinical psychiatry; it is intended for mental health professionals and for general clinical, educational and service use.
The CDDG does not provide diagnostic criteria. The essential features are less rigid than DSM-5’s criteria sets and allow practitioners more flexibility to use clinical discretion when making a diagnosis.
Qualified clinicians who signed up to participate in the CDDG guideline review process have been able to review and provide feedback on the draft content. No draft texts have been made available for public stakeholder scrutiny and comment and I have not had access, for example, to the most recent draft for the clinical descriptions and diagnostic guidelines for ICD-11’s Bodily distress disorder.
This paper in the February 2019 edition of World Psychiatry (Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders) describes major changes to the structure of the ICD‐11 classification of mental disorders as compared to ICD‐10; discusses new categories added for ICD‐11 and presents rationales for their inclusion; and describes important changes that have been made in each ICD‐11 disorder grouping [2].
What the paper does not give is a firm release date for the CDDG — stating only that the WHO will publish the CDDG as soon as possible following approval of the overall system by the World Health Assembly (WHA).
Member states approved the draft resolution to adopt ICD-11 at the 72nd World Health Assembly, in May 2019. Endorsement takes effect from January 01, 2022, which is the earliest date from which member states can begin reporting data using the new ICD-11 code sets.
Disorders of bodily distress and bodily experience
ICD‐11 disorders of bodily distress and bodily experience encompass two disorders: bodily distress disorder and body integrity dysphoria. ICD‐11 bodily distress disorder replaces ICD‐10 somatoform disorders and also includes the concept of ICD‐10 neurasthenia. ICD‐10 hypochondriasis is not included and instead is reassigned to the OCRD [Ed: Obsessive‐compulsive and related disorders] grouping.
Bodily distress disorder is characterized by the presence of bodily symptoms that are distressing to the individual and an excessive attention directed toward the symptoms, which may be manifest by repeated contact with health care providers69. The disorder is conceptualized as existing on a continuum of severity and can be qualified accordingly (mild, moderate or severe) depending on the impact on functioning. Importantly, bodily distress disorder is defined according to the presence of essential features, such as distress and excessive thoughts and behaviours, rather than on the basis of absent medical explanations for bothersome symptoms, as in ICD‐10 somatoform disorders.
DSM-5’s Somatic symptom disorder is listed under Synonyms to ICD-11’s Bodily distress disorder and indexed to 6C20.Z Bodily distress disorder, unspecified.
The CDDG is expected to be published as a licence free download. When the WHO has released the CDDG, I will update this post.
A majority of submissions regarding bodily distress disorder were critical, but were often made by the same individuals (N=8). Criticism mainly focused on conceptualization (48%; κ=0.64) and the disorder name (43%; κ=0.91). Use of a diagnostic term that is closely associated with the differently conceptualized bodily distress syndrome5 was seen as problematic. One criticism was that the definition relies too heavily on the subjective clinical decision that patients’ attention directed towards bodily symptoms is “excessive”. A number of comments (17%; κ=0.62) expressed concern that this would lead to patients being classified as mentally disordered and preclude them from receiving appropriate biologically-oriented care. Some contributors submitted proposals for changes to the definition (30%; κ=0.89). Others opposed inclusion of the disorder altogether (26%; κ=0.88), while no submission (κ=1) expressed support for inclusion. The WHO decided to retain bodily distress disorder as a diagnostic category6 and addressed concerns by requiring in the CDDG the presence of additional features, such as significant functional impairment.
Note: “Use of a diagnostic term that is closely associated with the differently conceptualized bodily distress syndrome5 was seen as problematic.”
Whilst it is welcomed that this specific concern has been acknowledged within this Letter to the Editor, I have drawn to the authors’ attention that WHO/ICD Revision has repeatedly failed to respond to requests to provide a rationale for its re-purposing of a diagnostic term that is already strongly associated with the Fink et al (2010) Bodily distress syndrome*, despite provision of examples from the literature clearly demonstrating that these two terms have been used interchangeably by researchers and practitioners, since 2007 [4].
The potential for confusion and conflation of these differently conceptualized disorder constructs was acknowledged by the WHO’s Dr Geoffrey Reed, in 2015. However, there has been no discussion of this potential in any of the S3DWG working group’s progress reports and field trial evaluations. If the WHO is not willing to reconsider and remedy this problem, there is the expectation that a rationale for going forward with the Bodily distress disorder term is provided for clinical and public stakeholders.
*Operationalized in Denmark and beyond, BDS is differently conceptualized to ICD-11’s BDD diagnostic construct: BDS has very different criteria/essential features, based on physical symptom patterns or clusters from organ systems; psychobehavioural responses to symptoms do not form part of the BDS criteria; BDS requires the symptoms to be “medically unexplained”; is inclusive of a different patient population to ICD-11’s BDD, and crucially, is considered by its authors to capture myalgic encephalomyelitis, chronic fatigue syndrome, IBS and fibromyalgia patients under a single, unifying BDS diagnosis.
As an unprocessed proposal is currently under review with the CSAC/MSAC committees I have requested that earlier submissions, which were marked as rejected in February 2019 with no adequate rationale for dismissing the concerns raised within them, are reconsidered and that the WHO responds to three specific concerns:
a) its re-purposing of a disorder term already in use interchangeably for a differently conceptualized disorder construct;
b) the potential difficulties of maintaining disorder construct integrity within and beyond ICD-11 and the implications for clinical utility, data reporting and statistical analysis;
c) the requirement for adding exclusions under BDD for Concept Title 8E49 Postviral fatigue syndrome and its inclusion terms, to mitigate confusion/conflation with the Fink et al (2007, 2010) Bodily distress syndrome.
Bodily distress disorder in SNOMED CT
The SNOMED CT Concept term SCTID: 723916001: Bodily distress disorder was added to the July 2017 release of the SNOMED CT International Edition.
SNOMED International’s classification leads confirmed that the term had been added by the team working on the SNOMED CT and ICD-11 MMS Mapping Project as “an exact match for the ICD-11 term, Bodily distress disorder.”
In ICD-11, Bodily distress disorder has specifiers for three degrees of severity: Mild BDD; Moderate BDD; and Severe BDD, which are each assigned a unique code and a discrete description/characterization text.
It was submitted that including the three ICD-11 BDD severities might help clinicians and coders distinguish between the SNOMED CT/ICD-11 Bodily distress disorder concept term and the similarly named, but differently conceptualized, Bodily distress syndrome (Fink et al 2010), which has two severities.
A request for addition of the three BDD severities was submitted and approved in early 2018 and Mild BDD; Moderate BDD; and Severe BDD were added as three discretely coded for Children concepts for the July 2018 release of the International Edition and subsequently absorbed into the various national editions.
ICD-11 PHC
The ICD-11 CDDG should not be confused with the ICD-11 PHC.
Since 2012, I have been reporting on the parallel development of the ICD-11 Primary Health Care (PHC) Guidelines for Diagnosis and Management of Mental Disorders (ICD-11 PHC).
The ICD-11 PHC is a revision of the Diagnostic and Management Guidelines for Mental Disorders in Primary Care: ICD-10 Chapter V Primary Care Version. 1996.
ICD-11 PHC is a clinical tool written in simpler language to assist non-mental health specialists in primary care settings and non medically trained health workers, and also intended for use in low resource settings and in low- to middle-income countries.
It comprises 27 mental disorders considered to be most clinically relevant in primary care and low resource settings. (It is a misnomer to refer to the ICD-11 PHC as the “Primary Care version of ICD-11” since it contains just 27 mental disorders and no general medical diseases or conditions.)
It is important to note that like the ICD-10 PHC, this revised diagnostic and management guideline won’t be mandatory for use by member states, although the WHO hopes this revised edition will have greater clinical utility than the ICD-10 PHC (1996).
The WHO intends to make the ICD-11 PHC publication, once completed, free to download by anyone. There is currently no date available for its projected finalization or release.
The revision is the responsibility of the WHO Department of Mental Health and Substance Abuse advised by an external advisory group — the Primary Care Consultation Group (PCCG) which is chaired by Prof Sir David Goldberg*; Vice-chairs: Dr Michael Klinkman and WHO’s, Dr Geoffrey Reed.
*Prof Sir David Goldberg also chaired the working group for the development of ICD-10 PHC (1996). Dr Michael Klinkman is a GP who represents WONCA (World Organization of Family Doctors) and current convenor of WONCA’s International Classification Committee (WICC) that is responsible for the development and update of the WHO endorsed, ICPC-2 (International Classification of Primary Care).
The full draft texts for the 27 mental disorder categories proposed for inclusion in the ICD-11 PHC have not been made available for public scrutiny, but a number of progress papers, field trial evaluations and presentations have been published since 2010 [5-8].
25 of the 27 mental disorder categories proposed for inclusion in the ICD-11 PHC have equivalence with mental disorder classes within the core ICD-11’s Chapter 06.
ICD-11 PHC is proposed to include a disorder category called “Bodily stress syndrome (BSS)” which replaces ICD-10 PHC’s “F45 Unexplained somatic complaints/medically unexplained symptoms” and “F48 Neurasthenia” categories.
This proposed “Bodily stress syndrome (BSS)” diagnosis has been adapted from the Fink et al (2010) Bodily distress syndrome (BDS). “Bodily stress syndrome (BSS)” does not have direct equivalence to a diagnostic construct in the core ICD-11.
The ICD-11 PHC’s “Bodily stress syndrome (BSS)” requires at least 3 persistent, medically unexplained symptoms, over time, of cardio-respiratory, gastrointestinal, musculoskeletal, or general symptoms of tiredness and exhaustion, that result in significant distress or impairment.
Under exclusions and differential diagnoses for BSS, certain psychiatric and general medical diagnoses have to be excluded but CFS, ME; IBS; and FM appear not to be specified as exclusions. So this (non mandatory) 27 mental disorder guideline needs very close scrutiny.
For the mandatory core ICD-11 classification, the WHO is going forward with the differently conceptualized, Bodily distress disorder (BDD), which has close alignment with DSM-5’s Somatic symptom disorder.*
If ICD-11 PHC goes forward with its proposed BSS category, there will be all these diagnostic constructs in play:
Somatic symptom disorder (DSM-5; under Synonyms to BDD in the core ICD-11) Bodily distress disorder (core ICD-11; SNOMED CT) Bodily stress syndrome (ICD-11 PHC guideline for 27 mental disorders) Bodily distress syndrome (Fink et al 2010, operationalized in Denmark and beyond)
plus the existing ICD-10 and SNOMED CT Somatoform disorders categories and their equivalents in ICPC-2.
3 Fuss J, Lemay K, Stein DJ, Briken P, Jakob R, Reed GM and Kogan CS. (2019). Public stakeholders’ comments on ICD‐11 chapters related to mental and sexual health. World Psychiatry, 18: 233-235. https://onlinelibrary.wiley.com/doi/full/10.1002/wps.20635
5 T P Lam, D P Goldberg, A C Dowell, S Fortes, J K Mbatia, F A Minhas, M S Klinkman. Proposed new diagnoses of anxious depression and bodily stress syndrome in ICD-11-PHC: an international focus group study, Family Practice, Volume 30, Issue 1, February 2013, Pages 76–87, https://doi.org/10.1093/fampra/cms037
6 MASTER PROTOCOL Depression, Anxiety and Somatic Symptoms in Global Primary Care Settings: A Field Study for the ICD-11-PHC Version 2 for WHO Research Ethics Review Committee.






{kind=link}
{kind=link}