Update to Letter to key Revision personnel re Continued absence of the ICD-10 G93.3 terms from the ICD-11 Beta drafting platform
June 22, 2015
Post #324 Shortlink: http://wp.me/pKrrB-46A
Update at February 23, 2016: Since no proposals and rationales for the ICD-10 G93.3 legacy terms were released in September or December 2015, I contacted ICD’s Dr Robert Jakob, again. Dr Jakob told me on February 2, 2016 that “[ICD-11 Revsion is] still working on the extensive review and the conclusions.”
This report is an update to Post #322:
Eight years into the revision process and stakeholders still don’t know how ICD Revision proposes to classify the ICD-10 G93.3 legacy terms for ICD-11.
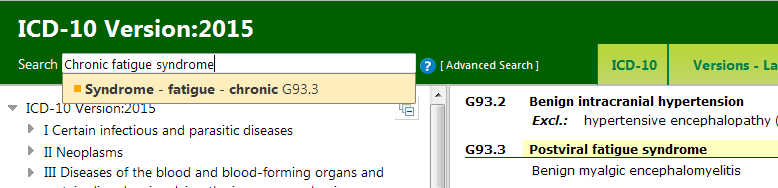
In ICD-10, the (G93.3) Title term is Postviral fatigue syndrome; Benign myalgic encephalomyelitis is the Inclusion term under G93.3; Chronic fatigue syndrome is included in the Index only, and indexed to the G93.3 code [1].
By 2012, the public version of the ICD-11 Beta draft had the three terms listed as in the screenshot, below – still under the Diseases of the nervous system chapter, but with a change of relationship between the three terms.
At that point, Chronic fatigue syndrome was being proposed as a new ICD Title term; Benign myalgic encephalomyelitis* was specified as the Inclusion term (indicated in the draft by hover text over the asterisk which is not displaying in this screenshot).
Postviral fatigue syndrome, previously designated as Title code in ICD-10, was now located under Synonyms, in a list of alternative and historical terms imported from other terminology systems and health informatics sources, including two terms specific to Chapter 18: Symptoms, signs etc. of the U.S. ICD-10-CM clinical modification [4].
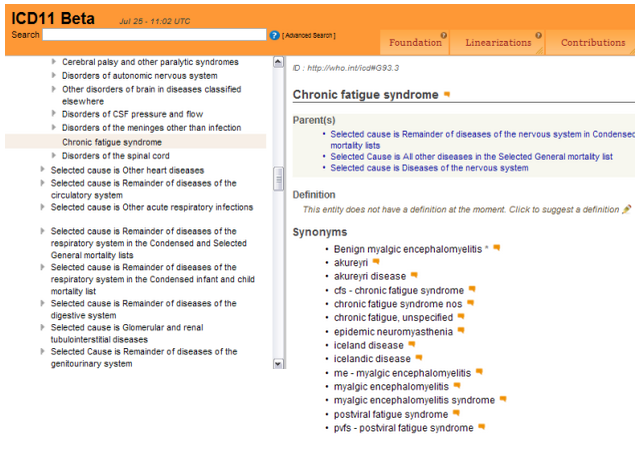
Source: ICD-11 Beta drafting platform, public version, July 25, 2012.
In early 2013, ICD Revision removed the entry for Chronic fatigue syndrome and its associated terms from the public version of the Beta draft; from that point on, none of the terms were accessible in any Linearization.
(In the version of the Beta that the public sees, there are no holding pens viewable for categories “Needing a decision to be made” and no tab for “Category Notes and Decisions” which might indicate the rationale for the temporary or permanent absence of a category from the draft.)
Although a Change History function was incorporated into the public Beta in March, no Change History is available for these terms. The Topic Advisory Group (TAG) for Neurology has published no progress reports on emerging proposals for scrutiny and discussion.
So for over 2 years, now, stakeholders have been unable to monitor evolving proposals for the classification of these G93.3 legacy entities within ICD-11. The continued absence of these terms hinders submission of comments and suggestions on proposed chapter location(s), parent classes, hierarchies, inclusions, exclusions, definitions or other Content Model descriptive text.
Request for release of information on current status of proposals
On June 8, I sent a letter to Bedirhan Üstün (WHO/ICD Revision Coordinator), Cc’d to key ICD Revision personnel and the recently assembled ICD Revision Project Management Team, requesting an update on the status of proposals for these terms and their restoration to the draft [5]. Read letter here
On Friday, June 19, Anneke Schmider (WHO Technical Officer, ICD Revision Project Manager) facilitated a conference call with myself and Dr Robert Jakob (WHO ICD classifications, ICD Revision Steering Group) in which Dr Jakob responded to my letter, having obtained a progress report from TAG Neurology.
NB: It was not the purpose of this discussion to advance my own views on how these terms should be represented within ICD-11 but to elicit clarifications on the current status of proposals.
Summary of main points from our discussion:
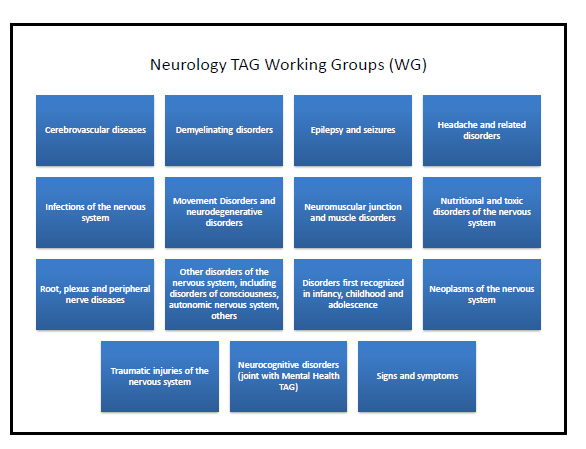
• TAG Neurology retains responsibility for these three terms.
• None of the sub-working groups that sit under TAG Neurology has specific responsibility for these terms.
• TAG Neurology is still reviewing the literature and has yet to reach consensus about where to classify these terms within ICD-11.
• Dr Jakob says he can be “crystal clear” that there is no proposal to classify the ICD-10 G93.3 legacy terms under the Mental and behavioural disorders chapter.
The ICD-11 principle of multiple parenting was discussed in general terms: multiple parenting allows the same disease to be expressed in two (or more) places in the ICD-11 linearizations. A disease or disorder category will be located under a primary parent class within one chapter but may also be searchable under a secondary (or tertiary) parent within another chapter, whilst retaining the code assigned in the primary location. (See ICD-11 Multiple parenting Slides 42-48)
Because TAG Neurology is still working towards consensus, Dr Jakob would not be drawn on the following:
• whether relocating one or more of these terms from the Diseases of the nervous system to an alternative chapter(s) was under consideration;
• whether retaining one or more of these terms within the Diseases of the nervous system chapter but secondary parenting under an alternative chapter(s) was under consideration;
• what existing parent classes were being considered for locating these terms under;
• whether the creation of any new parent classes was being considered for these terms;
• whether any changes in the relationship between the three terms, as they had stood in the Beta draft in early 2013, have already been agreed or remain under consideration (ie any changes to which of the terms are identified as ICD Title terms, which are specified as Inclusion terms and which are listed as Synonyms).
• which of the terms are proposed to be assigned a Definition and other Content Model descriptive text and where definition(s) would be sourced from.
It remains unclarified, therefore, whether ICD-11 intends to define CFS discretely from BME. Also unclarified: whether exclusions for these terms are proposed to be inserted under categories such as Bodily distress disorder; Fatigue [previously Malaise and fatigue in ICD-10]; and a proposed new Diseases of the nervous system parent term, Functional clinical forms of the nervous system (a proposal that TAG Mental Health opposes).
I have already submitted requests via the Proposal Mechanism that PVFS, BME and CFS are inserted under Exclusions to Bodily distress disorder, and Fatigue.
With regard to a date by which we might anticipate proposals being released:
• The Beta draft was frozen on May 31, 2015. The Beta Comment facility is open and stakeholders can register to comment on the draft or submit formal proposals for changes and enhancements to proposals via the Proposals Mechanism. Another frozen release is expected in August. (But while TAG Neurology’s proposals remain absent from the Beta and unpublished elsewhere, stakeholders are in no position to comment on the TAG proposals or submit suggestions for modifications to TAG proposals.)
• Dr Jakob says that in September 2015, ICD Revision plans to post various materials relating to the development process on the WHO/ICD website for public scrutiny, this to possibly include rationales, and documents relating to the abridged Primary Care version of ICD-11.
• If TAG Neurology’s proposals for the G93.3 legacy terms are not ready for September release, then Dr Jakob projected their release towards the end of December 2015.
• The target date for presentation of ICD-11 for World Health Assembly (WHA) approval is currently proposed for May 2018. There would be a period for public review and comment prior to presentation for adoption.
I will update on the status of proposals for these terms as soon as further information becomes available.
It is regrettable that stakeholders are little better informed than they were two years ago.
Bodily stress syndrome (S3DWG); Bodily stress syndrome (PCCG)
My longstanding concerns regarding the proposals of the WHO Working Group on Somatic Distress and Dissociative Disorders (S3DWG) for the revision of the ICD-10 Somatoform disorders and the alternative proposals of the ICD-11 Primary Care Consultation Group (PCCG) were beyond the scope of my letter to Dr Üstün and my discussions with Dr Jakob in response to that letter.
However, I advised Dr Jakob that my concerns around proposals for the S3DWG’s “Bodily distress disorder” and the Primary Care Consultation Group’s “Bodily stress syndrome” have been discussed with ICD Revision’s, Dr Geoffrey Reed, and in formal submissions via the Proposals Mechanism and Beta Comment facility for the consideration of TAG Mental Health [6][7].
References and related posts
1 ICD-10 Version: 2015 Chapter VI Diseases of the nervous system, G93.3
2 ICD-11 Beta drafting platform (Public version)
Frozen release at May 31, 2015
3 ICD-11 Beta Proposal Mechanism (Registration required for access)
4 Briefing paper on ICD-11 and PVFS, ME and CFS: Part 2, Dx Revision Watch
5 Continued absence of the ICD-10 G93.3 terms from the ICD-11 Beta drafting platform: Letter to key Revision personnel, Dx Revision Watch
6 Personal correspondence; ICD-11 Beta Proposal Mechanism.
7 Comment submitted to ICD-11 Topic Advisory Group for Mental Health re: Bodily distress disorder, Suzy Chapman





{kind=link}