Australian Senate seeks clarifications from ICD Revision
May 7, 2017
Post #337 Shortlink: http://wp.me/pKrrB-4iV
UK Parliamentary Questions
In February and March, the Countess of Mar tabled Written Questions in the House of Lords seeking clarifications from the World Health Organization (WHO) around ICD Revision’s proposals for the ICD-10 “legacy” terms, postviral fatigue syndrome, benign myalgic encephalomyelitis and chronic fatigue syndrome for ICD-11.
Both responses were as clear as mud and both refer to “chronic fatigue” – a term that exists neither in ICD-10 nor in ICD-11, and a term for which no proposal had been submitted.
You can view those Written Questions and Written Answers here:
HL5683
Written Question: 27 February 2017, Countess of Mar
Department of Health, Neurology
Written Answer: 07 March 2017, Lord O’Shaughnessy
HL6136
Written Question: 20 March 2017, Countess of Mar
Department of Health, Chronic fatigue syndrome
Written Answer: 28 March 2017, Lord O’Shaughnessy
Australian Senate also seeks clarifications
On March 29, Senator Griff (South Australian Senate) requested clarifications around the release date for ICD Revision’s proposals for the classification of the G93.3 legacy terms and the deadline for receipt of stakeholder comments.
A response was provided via the Minister of Health on April 28. These questions and responses will be recorded in the Australian Hansard.
In the context of the Australian Health Minister’s answers, please note the following and also the Notes beneath the copy of the Minister’s response:
1. When the G93.3 legacy terms were restored to the Beta draft on March 26 they were restored with this caveat:
While the optimal place in the classification is still being identified, the entity has been put back to its original place in ICD.
Team WHO 2017-Mar-26 – 12:46 UTC
2. From the Beta draft Proposal Mechanism (for which registration is required):
Deadline Information for proposals:
Deadline in order to be considered for the final version is 30 March 2017
Comments by Member States and improvements arising as a part of the Quality Assurance mechanism will be included with deadlines later in 2017
3. In this November 2016 slide presentation by WHO’s, Dr Robert Jakob, the deadlines for Member State comments and improvements arising as part of the Quality Assurance mechanism were given as:
2017 Deadline Members State comments (31 May )
2017 Deadline Field testing / quality assurance (30 June)
4. However, no public information has been available for the deadline for receipt of stakeholder comments in respect of proposals that met the March 30 deadline for consideration for inclusion in the final (2018) version.
Australian Senate Question and Response
SENATE QUESTION
QUESTION NUMBER: 435DATE ASKED: 29 March 2017
DATE DUE TABLING: 28 April 2017SENATOR Griff, asked the Minister representing the Minister for Health and Aged Care, upon notice, on 29 March 2017:
With reference to the World Health Organization (WHO) which is currently working on the latest edition of the International Classification of Diseases (ICD-11), and the Australian Collaborating Centre under the auspices of the Australian Institute of Health and Welfare which is coordinating Australia’s part in the latest edition:
1. Can the Minister request that the Joint Task Force responsible for steering the finalisation of the next edition of the WHO International Classification of Diseases to confirm the date by which the Topic Advisory Group for Neurology will release its proposals for the classification of the ICD-10 G93.3 legacy categories: post viral fatigue syndrome, benign myalgic encephalomyelitis and chronic fatigue syndrome, for public scrutiny and comment.
2. Can the Minister confirm the date by which comments on their proposals will be required to be submitted for the consideration of the Joint Task Force.
3. Can the Minister detail what the Australian Government is doing in terms of research into and treatment for post viral fatigue syndrome, benign myalgic encephalomyelitis and chronic fatigue syndrome.
SENATOR NASH – The Minister for Health has provided the following answer to the Honourable Senator’s question:
1. The World Health Organization (WHO) has released its classification of the International Classification of Diseases (ICD)-10 code G93.3 legacy categories (post viral fatigue syndrome, benign myalgic encephalomyelitis and chronic fatigue syndrome) in ICD-11; they are classified in the same way as they were in ICD-10*. This classification is visible in the draft of the ICD-11 that is available for comment on the WHO’s ICD-11 website. WHO has advised that the final classification in the ICD-11 will be decided based on an extensive scientific review.
WHO has been managing the development of ICD-11 with the advice from advisory groups including the Topic Advisory Group for Neurology and the Joint Task Force. The Topic Advisory Group for Neurology ceased operations in October 2016.
2. WHO has advised that comments on ICD-11 can be provided by anyone at any time through the ICD-11 website. Whilst the deadline for such comments to be made for consideration by WHO in the finalisation of ICD-11 for its release in 2018 was 30 March 2017, comments can be made after that date for consideration for future updates of ICD-11.
3. The National Health and Medical Research Council (NHMRC) has provided $1.6 million of research funding towards myalgic encephalomyelitis, chronic fatigue syndrome and other related fatigue states (ME/CFS) collectively since 1999.
NHMRC has created an online pathway for community and professional groups to propose ideas for health research topics and questions, which NHMRC may develop into a targeted call for research to invite grant applications. A targeted call for research is a one-time request for grant applications to advance research in a particular area of health and medicine that will benefit Australians. A submission on ME/CFS had been received through this pathway and is under consideration.
NHMRC staff are also in communication with the ME/CFS Action Group to discuss ways evidence based diagnostic and treatment advice can be adapted and applied in Australian clinical practice.
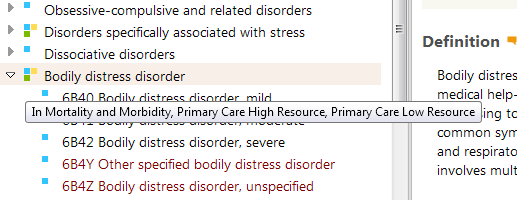
*Ed: The statement: “…[the terms] are classified in the same way as they were in ICD-10.” is not entirely correct. In ICD-10, chronic fatigue syndrome is not included in the Tabular List. It is listed in the Index, only, and points coders and clinicians to the G93.3 code. In the ICD-11 Beta listing for these terms, as restored (with a caveat) on March 26, both benign myalgic encephalomyelitis and chronic fatigue syndrome are specified as Inclusion terms to Postviral fatigue syndrome in both the ICD-11 Foundation and MMS Linearization (the ICD-11 equivalent of the Tabular List).
Notes:
This Australian Senate Response would appear to clarify the following:
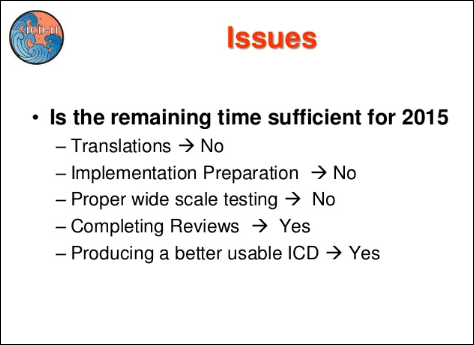
a) that despite nearly 10 years in development and with ICD-11 MMS due to be finalized by the end of this year, ICD Revision has still not reached consensus over the proposed classification of these three ICD-10 terms.
b) that the terms’ current placement and hierarchy in the ICD-11 Beta (as restored to the draft on March 26) may change between now and the end of this year or between now and the first scheduled annual maintenance and update revision (which would be expected in 2019, if ICD-11 is released in 2018).
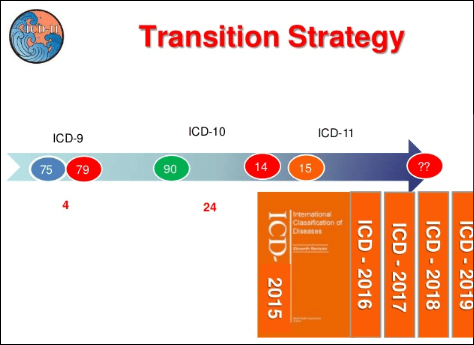
In order to be ready to present an initial version of ICD-11 to the WHA assembly in May 2018, the draft will need to be finalized by the end of 2017. See: Presentation with targets and timelines
If consensus were to be reached before the end of 2017, the Response does not clarify whether revised proposals would be entered into the Proposal Mechanism for public scrutiny and comment (or for how long) or would by-pass the Proposal Mechanism and be entered directly into the Beta draft as “Approved” and “Implemented” for incorporation into the final (2018) draft.
Or, having missed the March 30 deadline for consideration for inclusion in the initial 2018 release, whether any revised proposals released before the end of 2017 would need to be carried forward for consideration for inclusion in the first annual update in 2019, and if so, whether there would be any opportunity, at that stage, for stakeholder review and comment.
c) The response clarifies that the Topic Advisory Group for Neurology ceased operations in October 2016. Although it was understood that at some point the various Topic Advisory Groups would cease operating, the fact that TAG Neurology was no longer active was not communicated by Dr Robert Jakob or by the Joint Task Force to those of us attempting to obtain crucial information about proposals and deadlines via communications which, in some instances, the Chair of TAG Neurology (Dr Raad Shakir) was being copied into.
Two new ICD-11 advisory committees are expected to take over from the Joint Task Force:
Classification and Statistics Advisory Committee (CSAC) To perform as principal ICD-11 advisory committee, focusing mainly on ICD-11 MMS and its update proposals in mortality and morbidity
Medical and Scientific Advisory Committee (MSAC) To advise on scientific content for the ICD-11, of which advice is to be provided to CSAC
These advisory committees will be involved in the annual maintenance and update framework for ICD-11, once it has been released.
The Medical Scientific Advisory Committee (MSAC) was launched at the ICD-11 Revision Conference in 2016 and is expected to comprise approximately 6-10 experts selected by WHO. Dr Christopher Chute, who had chaired the ICD Revision Steering Group from 2010-2016, is a Co-Chair for the MSAC. Membership lists for MSAC and CSAC are not currently available and these new committees may still be in the process of being assembled.
It is possible that MASC and CSAC may be involved in final decisions about these terms, especially if consensus is not reached before the end of 2017.
Four day commenting window
The three terms were restored to the Beta draft on Sunday, March 26, when my long-standing proposals for exclusions under “Fatigue” were also partially approved and implemented, together with a somewhat opaque caveat posted by a Beta admin that prompted me to request clarification from Dr Jakob for its meaning.
Dr Jakob confirmed that the three terms had been restored to the Beta draft on March 26. But the restoration of the terms under parent, Other disorders of the nervous system was not viewable in the public version of the Beta until midday on Monday, March 27, because the public version of the platform had not been updated over the weekend and neither had the Print Versions or the Print Version of the Index.
This meant that having finally been restored to the draft, after a four year absence, the terms were viewable and open for comment by stakeholders for barely 4 days before the March 30 proposal and comment deadline was reached.
This also implies that several hundred stakeholder comments submitted after March 30 in response to the proposal submitted by myself and Mary Dimmock may have been submitted too late to be considered in the context of proposals that had met the March 30 deadline (which ours did) and may potentially be rolled forward for future consideration.
In February, I had asked Dr Robert Jakob and the Co-Chairs of the Joint Task Force three or four times if they would clarify by what date comments on proposals that met the March 30 deadline would need to be submitted – information that was vital for all public stakeholders planning to submit comment on Beta draft proposals – but these requests for clarification were sidestepped by both Dr Jakob and the Joint Task Force.
Stakeholders and stakeholder organizations should not be discouraged from submitting comments if they have not already done so.
The handling of these terms by ICD Revision (which included a four year period during which stakeholders were disenfranchised from the revision process – unable to scrutinize and comment on proposals because the terms had been inexplicably removed from the draft) and the cavalier and frequently obfuscatory manner in which stakeholder enquiries have been fielded, reflects very poorly on the WHO’s vision of an “open and transparent” revision process that is “inclusive of stakeholder participation” and on the WHO, in general.
PDF Questions tabled by Senator Griff (March 29, 2017) and Minister’s Response (April 28, 2017)
Key links
For a summary of our proposal and links for submitting comment via the Beta draft see: A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part Two



{kind=link}
{kind=link}