August 17, 2018
by admindxrw
Part One
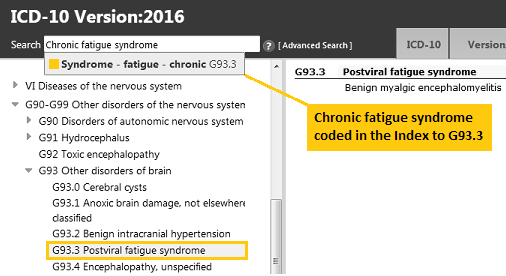
In the World Health Organization’s ICD-10, Postviral fatigue syndrome is classified in the neurological chapter of the Tabular List (at G93.3, under parent block: G93 Other disorders of brain, in Chapter VI: Diseases of the nervous system).
Benign myalgic encephalomyelitis is the inclusion term under Postviral fatigue syndrome and takes the same code. Chronic fatigue syndrome isn’t included in the Tabular List but is indexed in the Alphabetical Index to the G93.3 code.
ICD-10 and ICD-11 do not include the composite terms: “myalgic encephalomyelitis/chronic fatigue syndrome”, “ME/CFS” or “CFS/ME” and composite terms will not be used in this report.
This is how the terms appear in the online browser version of the ICD-10 Tabular List. If you enter “Chronic fatigue syndrome” into the Search field, a drop down displays the code that Chronic fatigue syndrome is indexed to:
http://apps.who.int/classifications/icd10/browse/2016/en#/G93.3
Release of ICD-11
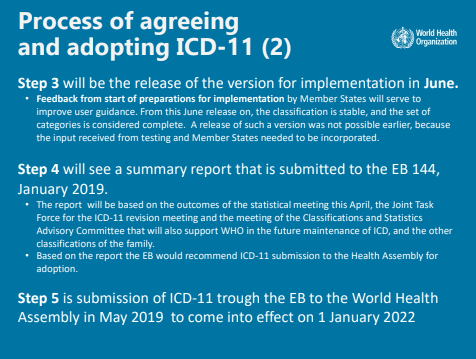
In Post #339 I reported on the release, in June 2018, of an “advance preview” version of ICD-11. This version has been released to enable countries to evaluate the new edition, plan for implementation, prepare translations and begin training health professionals. The WHO still has a lot of work to do before the full ICD-11 “implementation package” and companion publications are completed.
ICD-11 is scheduled for presentation at the World Health Assembly (WHA) in May 2019 for adoption by member states but WHA endorsement won’t come into effect until January 01, 2022. After that date, member states can begin using the new edition for data reporting — if their health systems are ready. There is no mandatory implementation date and member states will be migrating to ICD-11 at their own pace and according to their countries’ specific timelines, requirements and resources.
Update on classification for ICD-11
The progression of these three ICD-10 categories through the ICD-11 drafting process has been shambolic, mired in obfuscation, immensely frustrating for stakeholders — and still not resolved.
If you would prefer to jump to a report on how these three terms currently stand in ICD-11, as released in June 2018, and skip the key developments, go to Part Two
Key developments: tracking the progress of the ICD-10 G93.3 categories through the iCAT, Alpha and Beta drafting phases, between May 2010 and June 2018:
May 2010: The ICD-10 parent class, Other disorders of brain, is retired for ICD-11. Its retirement affects a number of categories that sit under it, not just Postviral fatigue syndrome.
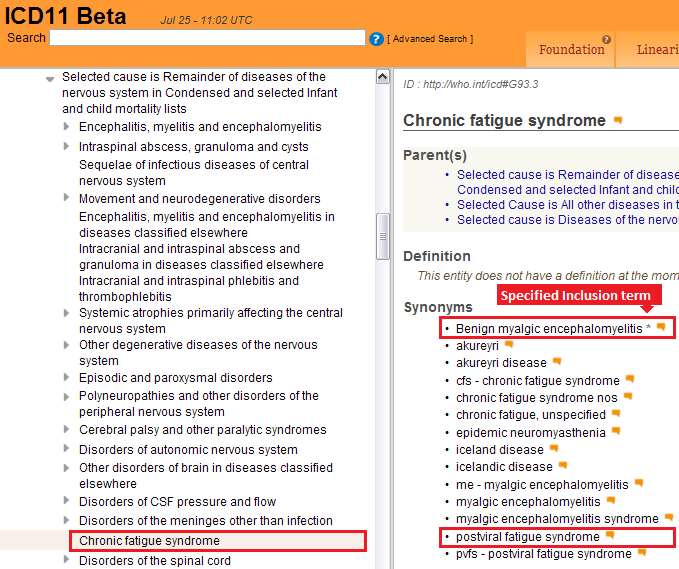
A change of hierarchy between the three terms is proposed (Screenshot).
Chronic fatigue syndrome is proposed to replace Postviral fatigue syndrome as the new “Concept Title” term, with Benign myalgic encephalomyelitis specified as its inclusion term (Screenshot). Postviral fatigue syndrome is proposed to be relocated under Synonyms to new Concept Title, Chronic fatigue syndrome.
All three terms are later removed from under parent block: Other disorders of the nervous system and placed in a “holding pen” for categories for which decisions are needed to be made or while further chapter restructuring is being carried out.
February 2013: The Beta drafting platform admins or the managing editors for Topic Advisory Group for Neurology inexplicably remove CFS, BME and PVFS from the public version of the Beta platform. No rationale is provided for their removal. No comments or suggestions for edits can be submitted for these terms since the terms are no longer displaying in the draft. This is how proposals for the terms had stood in early 2013, at the point at which they were removed from the public draft (Screenshot).
July 2015: Following a teleconference with the WHO’s Dr Robert Jakob and Anneke Schmider, Chapman and Dimmock provide ICD Revision and Topic Advisory Group for Neurology with a list of neurological and immunological studies and other resources to inform the revision process and the literature review.
February 2017: The three terms have now been missing from the public version of the Beta drafting platform for over four years.
Advocates and international patient organizations lobby the co-chairs and members of the ICD Revision Joint Task Force to place the matter of the continued absence of these terms from the public Beta draft on the agenda for the Joint Task Force’s February 20-22, 2017 meeting, in Cologne.
These appeals do result in the matter being tabled for discussion, as noted in the Meeting Report (Item 39, p39). But no immediate action is taken to restore the missing terms to the Beta draft and no progress report on intentions for these terms is forthcoming.
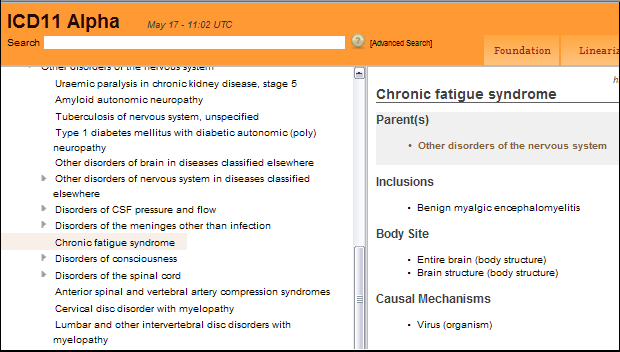
March 26, 2017: PVFS, BME and CFS are finally restored to the Beta draft under Other disorders of the nervous system, but with this caveat from the Beta draft admin team:
While the optimal place in the classification is still being identified, the entity has been put back to its original place in ICD. Team WHO 2017-Mar-26 – 14:46 UTC
PVFS is restored as the lead (Concept Title) term, as it is in ICD-10. BME and CFS are both specified as Inclusion terms. There is a list of around 15 alternative and historical terms under Synonyms and Index Terms — but “the optimal place in the classification is still being identified.”
At this point, ICD-11 has been under development for nearly ten years but Topic Advisory Group for Neurology has yet to publish any progress reports on its proposals for these ICD-10 categories.
This is how the terms stood after they were restored to the Beta draft in March 2017:

March 27, 2017: Suzy Chapman and Mary Dimmock finalize and submit a detailed proposal and rationale for PVFS, BME and CFS via the Beta draft proposal platform. This submission meets the March 30, 2017 proposal deadline. The proposal and rationale is supported by international patient organizations and patients. Click to download a PDF of the Proposal and Rationale.
(This proposal remains unprocessed and uncommented on by ICD Revision despite having met the proposal deadline.)
November 06, 2017: A new proposal for these terms is posted by Dr Tarun Dua.
Dr Dua is Medical Officer, Program for Neurological Diseases and Neuroscience, Management of Mental and Brain Disorders, WHO Department of Mental Health and Substance Abuse. This WHO department has responsibility for both mental disorders and neurological diseases. Its Director is Dr Shekhar Saxena.
Dr Dua had acted as lead WHO secretariat and managing editor to the Topic Advisory Group for Neurology, which had been chaired by Prof Raad Shakir.
It is initially unclear who owns this proposal and whose position it represents since Topic Advisory Group for Neurology had ceased operations in October 2016, leaving proposals for these terms hanging. We had been advised by the WHO several times since early 2017 that a literature review was still in progress:
Is this proposal the outcome of a now concluded literature review and do these recommendations already have the approval of ICD Revision?
Or does this proposal represent only the position of Dr Dua or the Department of Mental Health and Substance Abuse?
Four weeks after submitting these recommendations, Dr Dua responds:
“…the proposal has been submitted on behalf of Topic Advisory Group (TAG) on Diseases of the Nervous System, and reiterates the TAG’s earlier conclusions.”
but neither Dr Dua, Dr Saxena or (what remains of) TAG Neurology will provide any responses to requests for additional clarifications.
Dr Tarun Dua’s proposal
The proposal recommends that “Myalgic encephalitis/Chronic Fatigue Syndrome (ME/CFS)” [sic] should be removed from the Diseases of the nervous system chapter and reclassified in the Symptoms, signs chapter, as a child under Symptoms, signs or clinical findings of the musculoskeletal system.
Note that Dr Dua has not taken the existing ICD category terms as her reference point — ICD does not use the term, “Myalgic encephalitis” or the composite terms, “Myalgic encephalitis/Chronic Fatigue Syndrome” or “ME/CFS.”
It is not evident from the proposal what Dr Dua/TAG Neurology intends to do with the current Concept Title, Postviral fatigue syndrome — which the proposal does not mention, at all. Nor can it be determined what new hierarchy is being proposed between the terms. Nor is any rationale provided for using different nomenclature to the existing ICD terms.
Leaving aside the proposal, per se, the rationales that accompany it, the misconceptions contained within it and the narrow range of studies it relies on, the submission is sloppy and not fit for purpose.
The rationale for the proposal includes:
“…the lack of evidence regarding any neurological etiopathogenesis of chronic fatigue syndrome…
“When there is sufficient evidence and understanding of the pathophysiological mechanisms, diagnostic biomarkers, and specific treatments, the syndrome can be appropriately classified within the proper block.
“The predominant symptom of those with ME/CFS present is severe fatigue, a manifestation of skeletal muscle dysfunction…
“Epidemiological and Pathophysiological evidence is limited, conflicting, and does not support ME/CFS as a disease of the nervous system or with a principally neurobiological underpinning…
“ME/CFS is thus not a disease of the nervous system. It should be categorized in the Signs and Symptoms chapter given the lack of clear evidence pointing to the etiology and pathophysiology of this syndrome until evidence to organ placement is clarified in years to come.”
Click here to read the full proposal Dr Dua November 06, 2017. (If you are not registered for access to the proposals platform, a copy of Dr Dua’s proposal is included at the end of this commentary for ease of access.)
One also has to question why this proposal was submitted at this point when advocates had been advised several times that an in-house evidence review was in progress.
This proposal from a staffer in the Department of Mental Health and Substance Abuse (submitted apparently on behalf of a retired external advisory group) appeared to sit outside that evidence review. But when questioned about the proposal’s status, no-one within WHO seemed to want to have to acknowledge its existence or clarify whether and how it related to the evidence review.
Lack of consensus between WHO staffers and ICD Revision
In March 2017, Dr Robert Jakob, Team Leader Classifications and Terminologies, had given the assurance, via an email sent to Suzy Chapman (Dx Revision Watch) and CCd to Stefanie Weber; Dr Christopher Chute; Linda Best; Molly Meri Robinson Nicol; Dr Geoffrey Reed; Dr Tarun Dua; Dr Ties Boerma and the Countess of Mar, that:
“As discussed earlier, chronic fatigue syndrome will not be lumped into the chapter ‘signs and symptoms.'”
Yet this proposal submitted by Dr Dua proposes to do just that.
Evidently, there is a lack of consensus between the WHO’s senior classification lead, Dr Robert Jakob, and Dr Dua/TAG Neurology.
Dr Dua’s proposal also fails to take into consideration WHO/ICD-11 guiding principles on relocation of legacy terms to other chapters. For an expanded commentary on ICD-11 principles concerning potential relocations see Extract from Response to Dr Dua Proposal of November 6 2017.
Nor do the recommendations consider any proposed relocation in the context of data collection, statistical analysis and backward compatibility with ICD-10 and its clinical modifications.
To continue with the status of these terms in the ICD-11 draft, up to its release in June 2018, go to Part Two
References:
1 G93.3 Postviral fatigue syndrome, ICD-10 Browser Version: 2016. Accessed August 14, 2018
2 World Health Organization finally releases next edition of the International Classification of Diseases (ICD-11) Dx Revision Watch, July 25, 2018
3 8E49 Postviral fatigue syndrome, ICD-11 for Mortality and Morbidity Statistics (ICD-11 MMS) 2018 version for preparing implementation. Accessed August 14, 2018
4 8E49 Postviral fatigue syndrome, ICD-11 (Mortality and Morbidity Statistics) Maintenance Platform. Accessed August 14, 2018 The content made available here is not a released version of the ICD-11. It is a work in progress in between released versions.
5 ICD Revision Joint Task Force Meeting Report 22-22 January, 2017, Cologne, Germany. Page 39, Item 39: Chronic Fatigue Syndrome Advocacy Efforts. Accessed August 14, 2018
6 A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part Two. Dx Revision Watch, April 3, 2017
PDF: Proposal: Revision of G93.3 legacy terms for ICD-11, Dimmock & Chapman, March 27, 2017
7 Proposal: Revision of G93.3 legacy terms for ICD-11, Dr Tarun Dua, November 6, 2017
8 Response by Dimmock & Chapman to Dr Tarun Dua proposal of November 6, 2017, February 15, 2018
9 ICD-11 Reference Guide June 2018
10 Extract from Response to Dr Dua Proposal of November 6 2017: 4. Compliance with WHO standards and other considerations on relocation, Dimmock & Chapman, February 15, 2018








{kind=link}
{kind=link}
{kind=link}