July 29, 2012
by meagenda
ICD-11 Revision Beta drafting process: stakeholder participation
Post #194 Shortlink: http://wp.me/pKrrB-2nw
Information in this report relates to the World Health Organization’s ICD-11, currently under development. It does not apply to the existing ICD-10 or to the forthcoming US specific “clinical modification” of ICD-10, known as ICD-10-CM.
Update at August 2, 2012:
ICD-11 Slide Presentation:  Harrison Slides 2011 PDF 3MB
Harrison Slides 2011 PDF 3MB
+++
Update at August 2, 2012:
Dr Robert J.G. Chalmers, co-chair and managing editor of ICD Revision Dermatology Topic Advisory Group put out a call, yesterday, on the website of the American Academy of Dermatology Association (AAD) for input into the Beta draft for Chapter 12 Diseases of the skin:
An invitation to contribute to the future of dermatology
ICD-11 Update
By Robert J.G. Chalmers
ICD-11 draft is ready for comments and criticism
By Robert J.G. Chalmers, MB, FRCP, August 01, 2012
+++
When will ICD-11 be ready for dissemination?
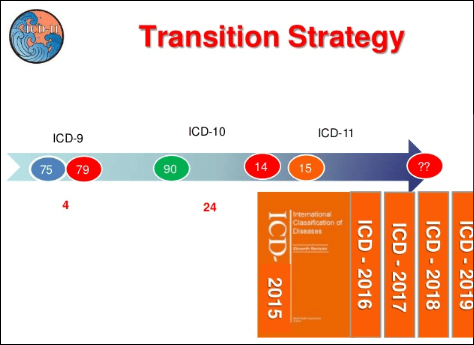
Slipping targets
The revision of ICD-10 and development of the structure for ICD-11 began in 2007.
ICD-11 was originally planned to be ready for dissemination by 2012, with the timelines for the revisions of ICD-10 and DSM-IV running more or less in parallel. Source: Archive documents, References [1] [2].
Very early on in the revision process, the ICD-11 dissemination date was extended from 2012 to 2015. In 2009, launch of the Beta draft was timelined for May 2011, with the final draft scheduled for submission to World Health Assembly (WPA) for approval in 2014.
In order to be ready for global implementation in 2015, the technical work on ICD-11 would need to be completed by 2012. Source: Dr Geoffrey Reed, Ph.D., May 2009, via personal correspondence.
+++
ICD-11 still at the Beta drafting stage
In early 2011, in response to slipping targets for content population and software development, ICD Revision and WHO-FIC were discussing the pros and cons of postponing the launch of a Beta drafting platform until later that year or until May 2012, and whether an interim solution might be to launch “a hybrid model of opening the revision process to public comment and suggestions at the same time not a full scale beta phase with field trials…”

Sources: Slide presentation: ICD Revision Paediatrics Meeting, Ankara, Turkey, February 28 – March 1, 2011;
Report: WHO-FIC Council conference call, February 16, 2011: Page 6: PDF for Report [3]
+++
Launch of the Beta delayed
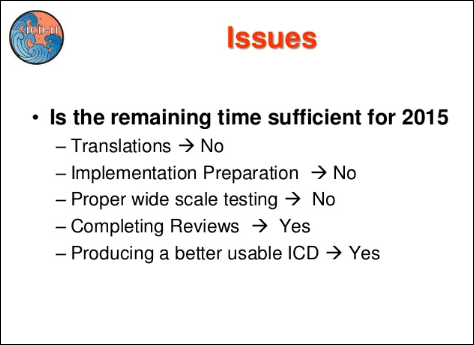
The decision was made to delay launching the Beta draft until May 2012. With the Alpha and Beta stages already running a year or more behind 2009 targets, it’s not clear how much time can be allocated for completing the Beta phase and two year field trials period – if the target for a final version for public viewing in 2014 is going to be reached.
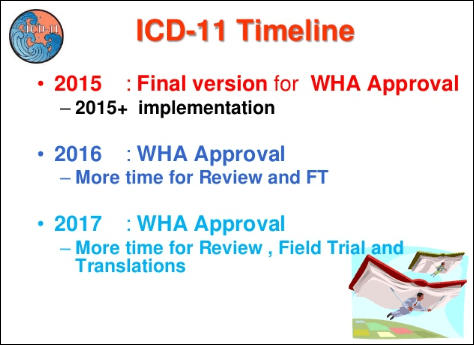
According to the ICD-11 Timeline, presentation for World Health Assembly approval has been shifted to May 2015 and in this paper, published in March 2012 by Christopher Chute, MD, (Chair, ICD-11 Revision Steering Group) et al, publication of ICD-11 is now expected “around 2016.”
+++
“…And just a small detail: who will do all this work?” [4]
ICD-11 is a very ambitious project.
The burden of drafting and liaison is being carried out largely via electronic means between individuals scattered across the globe and in addition to their clinical and academic responsibilities.
Given the scale of the undertaking, its technical complexity, limited funding and human resources, lack of an overall project manager, reported communication problems between WHO, Revision Steering Group, Topic Advisory Group managing editors and members and the amount of work that remains to be completed, I cannot see this vision of WHO’s Bedirhan Üstün reaching fruition by 2016.
There are some interesting comments in this Agenda Appendix (Page 6 of 10) on project funding, lack of resources, project management and lines of communication: ICD-11 April 11 Meeting Agenda
For make-up of the Revision Steering Group (RSG) and the various Topic Advisory Groups (TAGs) see links at end of post. Membership of the various sub working groups to Topic Advisory Groups and the names of external peer reviewers of proposals and content have not been published by ICD-11 Revision.
+++
Where can the Beta drafting platform be viewed?
ICD Revision Steering Group and the various Topic Advisory Groups that are developing the Beta draft are working on an electronic collaborative authoring platform, called the iCAT, on a password protected server accessible only by WHO classification experts, Revision Steering Group, Topic Advisory Group Managing Editors and revision process IT personnel and software developers. It looks similar to this:

For more views of the iCAT see Slides 20-25 and Slide 39 of this 2011 slide presentation:
ICD-11 Slide Presentation:  Harrison Slides 2011 PDF 3MB
Harrison Slides 2011 PDF 3MB
The iCAT platform is more complex than the publicly viewable version of the Beta platform and has a mechanism for recording change histories which tracks additions, deletions and revisions to the draft as ICD chapters are reorganized and new content generated and populated.
Population of content is managed by the Topic Advisory Group (TAG) Managing Editors following review by the Revision Steering Group. Structural changes to the classification, eg changing parent/child relationships and editing the linearizations can only be done by TAG Managing Editors in liaison with WHO classification experts. Source: Drafting Workflow text and chart [MS Word]; Swim Lane Workflow chart [PDF].
The publicly viewable version of the Beta drafting platform, which was launched in May 2012, looks like this:

With no change histories displaying in the public version of the Beta it is difficult for stakeholders to track proposed hierarchical changes to existing categories, changes to the names of parent classes or child categories, proposed introduction of new category terms (and the rationales for these) or proposed retirement of ICD-10 categories.
In the absence of rationales, it cannot be determined whether the disappearance of a category or group of categories is due to error or oversight by Advisory Group Managing Editors or others with editor level access, a temporary absence while a specific chapter section is being reorganized or whether these no longer displaying categories are intended to be subsumed under existing or new categories.
For example, a number of ICD-10 F45 and F48 Somatoform Disorder categories were removed from the Beta draft in early July with no explanation of intention.
Whilst ICD Revision invites interaction with the drafting process, the lack of clear intent on the part of Advisory Group editors and lack of response to requests for clarifications hinder submission of meaningful stakeholder comment and productive interaction with the process.
Caveats
When viewing the Beta draft, be mindful of the Caveats published by ICD Revision; the draft is in a state of flux.
The ICD-11 Beta drafting process is a work in progress over the next two to three years. The Beta draft is updated on a daily basis to reflect the work being carried out on the iCAT platform. Parent terms, category terms and sorting codes assigned to categories are subject to change as chapter reorganization progresses.
The Beta draft can be accessed here:
Beta draft Foundation Component (FC) view:
http://apps.who.int/classifications/icd11/browse/f/en
Beta draft Linearization Morbity (LM) view:
http://apps.who.int/classifications/icd11/browse/l-m/en
For definitions of Synonyms, Inclusions, Exclusions and ICD-11 terminology see the iCAT Glossary.
+++
Who are the stakeholders in ICD?
government service providers
policy makers and policy implementation agencies
health care professionals and practitioners
physician groups, especially primary care physicians
psychiatrists
psychologists
nurses
researchers and clinician academics
lay health care workers (who deliver most of the primary and mental health care in some developing countries)
social workers
patients (aka service users/consumers of health services), their families and carers
advocacy and disability rights organizations
health information managers and coders
health information technology workers
insurers
On its Facebook page, in June, ICD Revision put out a specific call for professionals with backgrounds in the following fields:
http://www.facebook.com/ICD11
Do you have a background in any of the following areas?
Medicine
Nursing
Midwifery
Dentistry
Pharmacy
Health information management (coding, medical records)
Environmental and occupational health and hygiene
Physiotherapy or Physical therapy
Nutrition
Social Sciences
Psychology
Social work and counseling
Epidemiology
Health Policy
Traditional and complementary medicine
WHO is asking experts from all over the world to sign up today to participate in the ICD revision.
www.who.int/classifications/icd11
+++
How can stakeholders participate in the Beta process?
The public version of the Beta platform can be viewed without registration.
Professional stakeholders and others who register an interest are able to interact with the drafting process and have access to additional content.
Interested stakeholders can register here
Registered stakeholders are permitted to:
• Add comments on and read other stakeholder comments on concepts; title terms; synonyms; inclusion terms, exclusions and other Content Model parameter terms;
• Comment on whether a category is in the right place;
• Comment on whether the category is useful for Primary Care; Research; Clinical;
• Suggest definitions (with source for definition) for a disease or disorder and comment on already populated draft definitions;
• Make proposals to change ICD categories;
• Offer to participate in field trials (for professionals);
• Offer to assist in translating ICD into other languages
Comments left by registered stakeholders are not visible to non registered viewers. Comments cannot be edited or deleted and appear immediately.
Recent comments get aggregated here:
http://apps.who.int/classifications/icd11/browse/Contributions/RecentComments
+++
PDFs of Print Versions for the ICD-11 Beta Morbidity Linearization
Registered users can download individual chapters or the full linearization using the links on this page. These PDF files are updated every few days to reflect the daily revisions to the drafting platform:
http://apps.who.int/classifications/icd11/browse/l-m/en/Printables
For more information on how it is envisaged professional and lay stakeholders will interact with the drafting process see:
PowerPoint presentation slides in Posts #70 and #71:
ICD Revision Process Alpha Evaluation Meeting 11 – 14 April 2011: The Way Forward?
ICD Revision Process Alpha Evaluation Meeting documents and PowerPoint slide presentations
ICD-11 Revision Video invitation to participate here: Video invitation to participate
Press Release here announcing launch of Beta drafting platform. Further media coverage here
Specific call for comments from neurology professionals on The Lancet Neurology site here:
http://www.thelancet.com/journals/laneur/article/PIIS1474-4422(12)70125-4/fulltext
+++
Recently issued documents around the Beta drafting process
Frequently Asked Questions About ICD-11
ICD-11 Beta: Expectations, Concerns and Known Issues: Information for Beta Participants
http://www.who.int/classifications/icd/revision/betaexpectations/en/
ICD-11 Known Concerns and Criticisms: Known concerns about the ICD-11 Beta phase
http://www.who.int/classifications/icd/revision/icd11betaknownconcerns.pdf
ICD-11 Beta known concerns
ICD-11 Known Problems and Issues: General known issues
http://www.who.int/classifications/icd/revision/icd11knownissues.pdf
ICD-11 General known issues
+++
The ICD-11 Content Model
ICD Revision says that the most important difference between ICD-10 and ICD-11 will be the Content Model.
In ICD-10, other than Chapter V Mental and behavioral disorders, there are no definitions or other descriptive content associated with ICD categories – just hierarchical lists of diseases arranged by chapter and their ICD codes.
But content in ICD-11 is being populated in accordance with the Content Model Reference Guide and there will be the potential for considerably more content to be included for diseases, disorders and syndromes in ICD-11 than appears in ICD-10, across all chapters:
“Population of the Content Model and the subsequent review process will serve as the foundation for the creation of the ICD-11. The Content Model identifies the basic characteristics needed to define any ICD category through use of multiple parameters.”
The most recently published version of the Content Model Reference Guide is here:
Content Model Reference Guide January 2011 [MS Word]
There are currently 13 defined parameters in the content model to describe a category in ICD. All categories will have an ICD Entity Title, Classification Properties, Textual Definition, Terms and up to 13 parameters described.
Content Model Parameters
- ICD Entity Title
- Classification Properties
- Textual Definitions
- Terms
- Body System/Structure Description
- Temporal Properties
- Severity of Subtypes Properties
- Manifestation Properties
- Causal Properties
- Functioning Properties
- Specific Condition Properties
- Treatment Properties
- Diagnostic Criteria
Some ICD-11 chapters are more advanced than others for reorganization of categories and population of proposed definitions and text for other parameters.
In setting itself the task of generating, peer reviewing, populating and approving this amount of detail across the entire ICD, one has to question how realistic a goal this is within current timeframes.
“Populating the Content Model is a critical task for the revision. Failure results in failure of delivery of ICD‑11.” [4]
It would not surprise me if at some point before the end of this year, ICD Revision Steering Group announces further delays for the Beta drafting and field trial stages and an extension to the projected dissemination date, or a scaling back of the project if completion of ICD-11 and its several, planned speciality publications, by 2016, is to be viable.
+++
Will ICD-11 be implemented worldwide from 2015/16?
ICD-10 is used in over 100 countries, worldwide. Assuming ICD-11 does meet it schedules, it may still take several years before countries currently using ICD-10 are ready to adopt ICD-11.
Several countries have been authorized by WHO to develop their own “Clinical Modification (CM)” of ICD. Canada uses an adaptation called ICD-10-CA, with a version published for 2009. Germany uses a version called ICD-10-GM. Australia (ICD-10-AM) and Thailand (ICD-10-TM) also use country specific modifications of ICD-10.
The US lags behind the rest of the world and is still using a CM version of ICD based on the ICD-9, which is long since retired by the WHO.
Instead of moving onto ICD-11, once this is completed, the US had scheduled implementation of a clinical modification of ICD-10 called ICD-10-CM, for October 1, 2013. ICD-10-CM has been in development for a considerable number of years.
On April 17, 2012 the Secretary of HHS issued a proposed rule to delay the compliance date for ICD-10-CM and ICD-10-PCS codes sets from October 1, 2013 to October 1, 2014, in order to allow more time for clinical practices and the coding industry to prepare for transitioning from ICD-9-CM to ICD-10-CM.
The public comment period for the proposed rule to delay the compliance date is now closed and comments are in the process of being reviewed. A final rule has yet to be announced. Until a new compliance date has been ratified and the revised implementation date reached, codes in ICD-10-CM are not valid for any purpose or use but can be viewed for free on the CDC website together with other ICD-10-CM documentation.
The US might not anticipate moving on to a clinical modification of ICD-11 before 2020 and possibly later*.
*Source: DHSS Office of Secretary Final Rule document: “We estimated that the earliest projected date to begin rulemaking for implementation of a U.S. clinical modification of ICD–11 would be the year 2020.”
WHO-FIC meeting materials suggest no earlier than 2018 for Canada. Australia is discussing earlier adoption of ICD-11 (or a CM of ICD-11).
Harmonization between ICD-11 and DSM-5
There is already a degree of correspondence between DSM-IV categories and Chapter V of ICD-10. For the next editions, the APA and WHO have committed as far as possible:
“To facilitate the achievement of the highest possible extent of uniformity and harmonization between ICD-11 mental and behavioural disorders and DSM-V disorders and their diagnostic criteria.”
with the objective that
“The WHO and APA should make all attempts to ensure that in their core versions, the category names, glossary descriptions and criteria are identical for ICD and DSM.”
WHO acknowledges that there may be areas where congruency may not be achievable.
With the timelines for DSM-5 and ICD-11 running out of synch (DSM-5 slated for publication in May 2013; ICD-11 still at the Beta drafting stage with a two year period scheduled for completion of its field trials), this may present barriers to harmonization.
In a June 2011 presentation to the International Congress of the Royal College of Psychiatrists, APA President, John M. Oldham, MD, MS, spoke of “Negotiations in progress to ‘harmonize’ DSM-5 with ICD-11 and to ‘retro-fit’ these codes into ICD-10-CM” and that DSM-5 would need “to include ICD-10-CM ‘F-codes’ in order to process all insurance claims beginning October 1, 2011.”
With the three systems: DSM-5 (publication date May 2013), ICD-10-CM (subject to partial code freeze since October 1, 2011 until 2014+ with new compliance date t.b.a.) and ICD-11 (dissemination scheduled for 2015+) set to become potentially more closely aligned, proposals for ICD-11 may have implications for US health care professionals and patient populations who might also consider themselves stakeholders in the ICD-11 development process.
+
References and additional ICD-11 related links and documentation
According to documents [1] and [2], ICD-11 was originally planned for dissemination by 2012, with the timelines for revisions of ICD-10 and DSM-IV running more or less in parallel. By 2008, the completion date for ICD-11 had been extended to 2014. In December 2009, the American Psychiatric Association (APA) announced a shift in the publication date for DSM-5 to May 2013. APA News Release No. 09-65
1] IUPsyS Mar 08 Agenda Item 25 ICD-10
International Union of Psychological Science COMMITTEE ON INTERNATIONAL RELATIONS ACTION, March 28–30, 2008, Agenda Item No. 25: Revision of the International Classification of Diseases (ICD-10) and Involvement of Psychology
2] Exhibit 1 WHO Letter Aug 07
Letter Saxena, WHO, to Ritchie, IUPsyS (International Union for Psychological Science), August 2007
Source: http://www.apa.org/international/governance/cirp/s08agenda25-Exhibit1.pdf
3] Pages 5-6: Report, WHO FIC Council conference call, 16 February 2011, PDF format
4] Closing remarks, PowerPoint presentation: “Proposal for the ICD Beta Platform”, Stanford team, 12.04.11, WHO, Geneva.
5] Key document: ICD Revision Project Plan version 2.1 9 July 2010
Key links
ICD-11 Beta drafting platform | Publicly viewable version
WHO ICD Revision | Main WHO website: Revision Steering Group and Topic Advisory Groups
ICD-11 Revision site | Revision resources [Google site currently unavailable]
ICD-11 Revision site Documents Page | Key revision documents and meeting materials [Google site currently unavailable]
ICD-11 Revision Information |
ICD-11 Timeline |
ICD Information Sheet |
Revision News |
Steering Group |
Topic Advisory Groups |
ICD-11 YouTube Channel | Video reports
ICD-11 on Facebook |
ICD-11 on Twitter |
ICD-11 Blog | Not updated since October 2009
ICD-11 YouTubes collated on Dx Revision Watch ICD-11 YouTubes |
WHO Publications
ICD-10 Tabular List online Version: 2010 | International Statistical Classification of Diseases and Related Health Problems 10th Revision Version: 2010, Tabular List of inclusions and Chapter List
ICD-10 Volume 2: Instruction Manual | Volume 2 online Version: 2010 PDF Download
ICD-10 for Mental and Behavioural Disorders Diagnostic Criteria for Research | PDF download
ICD-10 for Mental and Behavioural Disorders Clinical Descriptions and Diagnostic Guidelines | PDF download
ICD-10 Volume 3: The Alphabetical Index | WHO does not make ICD-10 Volume 3: The Alphabetical Index available online
About the World Health Organization (WHO)
The WHO Family of International Classifications
History of ICD