A round up of updates on ICD-11
August 6, 2020
Post #360 Shortlink: https://wp.me/pKrrB-59G
1. Next release of the ICD-11 MMS (the blue “Version for preparing implementation” platform)
It was anticipated that the ICD-11 Blue platform would continue to be updated annually to incorporate all the changes approved and implemented in the Orange Maintenance platform since the last update was released.
There has been no new release of the Blue platform since April 2019.
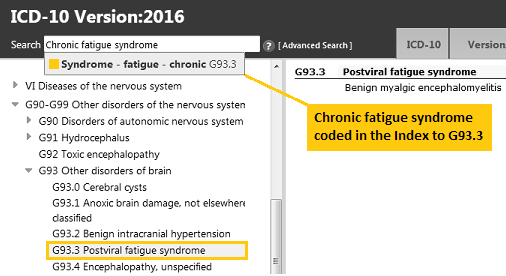
So, for example, the exclusions for 8E49 PVFS; BME; and CFS under 6C20 Bodily distress disorder, which were approved and implemented in the Orange Maintenance platform in January, this year, don’t yet display under the exclusions list for 6C20 Bodily distress disorder in the Blue platform.
A couple of weeks ago, I contacted the WHO’s Dr John Grove to enquire when the next update of the Blue platform was anticipated to be published.
I also asked when the Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders is expected to be finalised and released.
Yesterday, I received a response from the WHO’s Dr Robert Jakob who advised that the 2020 release of the ICD-11 Blue platform will be posted in a few weeks.
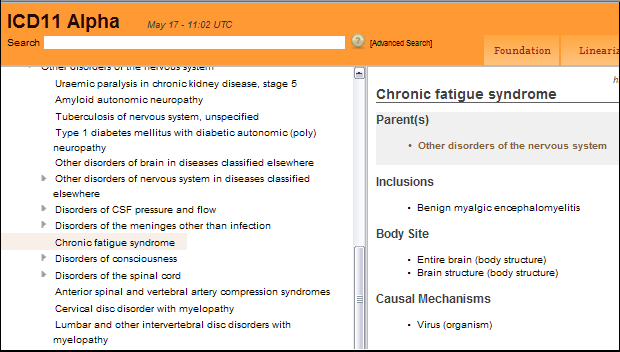
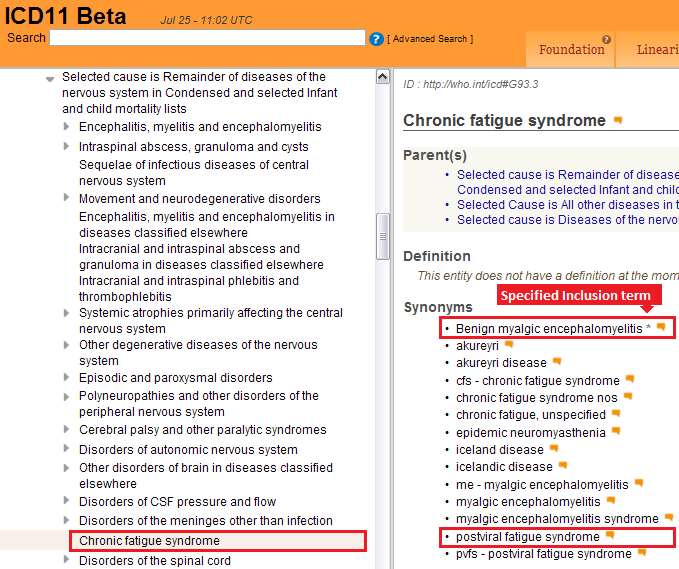
2. Proposal for deprecation of the prefix “Benign” from “Benign myalgic encephalomyelitis”
In February, I submitted a new proposal for removal of the prefix “Benign” from “Benign myalgic encephalomyelitis” citing, inter alia, the precedent of the removal of the “Benign” prefix for the final update of ICD-10 (Version: 2019).
My proposal and rationale can be read here in PDF format.
There remain hundreds of proposals waiting to be reviewed in the ICD-11 Proposal Mechanism and my proposal has not yet been processed. I am hoping it will be reviewed and accepted in time for inclusion in the ICD-11 MMS 2020 release.
3. Finalisation and publication of the CDDG
The Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD-11 Mental, Behavioural and Neurodevelopmental Disorders has been developed by the WHO Department of Mental Health and Substance Abuse. It is the equivalent of the ICD-10 “Blue Book”.
The descriptive texts in Chapter 06: Mental, behavioural or neurodevelopmental disorders in the core version of ICD-11 are intended for use by coders and clerical workers as a basis for statistical reporting.
The CDDG provides expanded clinical descriptions, essential (required) features, boundaries with other disorders and normality, differential diagnoses, additional features, culture-related features and codes for all mental and behavioural disorders commonly encountered in clinical psychiatry and is intended for use by mental health professionals and for general clinical, educational and service use.
The draft texts for the CDDG have not been accessible to public stakeholders for review and comment, though clinicians have been able to register to review the draft and provide feedback throughout its development, via the Global Clinical Practice Network platform.
Last year, the WHO stated that the CDDG would be published “as soon as possible” after the May 2019 adoption of ICD-11 at the 72nd World Health Assembly.
I was advised, yesterday, by Dr Jakob, that the CDDG is still being amended based on feedback from the field and that the mental health team hasn’t provided a clear deadline [for its finalisation and release].
4. Publication of the ICD-11 PHC
There is no indication when the WHO expects to finalise and release the ICD-11 PHC — a clinical guideline written in simpler language to assist non-mental health specialists, especially primary care practitioners and non medically trained health workers and also intended for use in low resource settings and low- to middle-income countries, with the diagnosis and management of common mental disorders.
The ICD-11 PHC is proposed to comprise 27 mental disorders and contains no general medical diseases. Like the ICD-10 PHC (1996), this revised diagnostic and management guideline will not be mandatory for use by member states.
For the mandatory core ICD-11 classification, the WHO has gone forward with Bodily distress disorder (BDD), which is conceptually similar to DSM-5’s Somatic symptom disorder (SSD).
But for the ICD-11 PHC, a disorder category called “Bodily Stress Syndrome (BSS)” that has been adapted from the Fink et al (2010) Bodily distress syndrome (BDS) is proposed to be included to replace ICD-10 PHC’s F45 Unexplained somatic complaints and F48 Neurasthenia categories.
See Comparison of SSD, BDD, BDS, BSS in classification systems, July 2018.
Under exclusions and differential diagnoses for BSS, certain psychiatric and general medical diagnoses have to be excluded but CFS, ME; IBS; and FM appear not to be specified as exclusions.
For more information on the ICD-11 PHC see this post: Clinical Descriptions and Diagnostic Guidelines (CDDG) for ICD‐11 Mental, Behavioural and Neurodevelopmental Disorders
Slide presentation: MUS becomes Bodily Stress Syndrome in the ICD-11 for primary care, Marianne Rosendal
The ICD-11 PHC has not been developed on a publicly accessible platform and the draft texts for the 27 mental disorders proposed to be included are not available for public stakeholder review and comment.
The “Bodily Stress Syndrome (BSS)” category, its proposed text and proposed criteria need stakeholder scrutiny.
If ICD-11 PHC goes forward with its proposed BSS category, there will be all these diagnostic constructs and criteria sets in play:
Somatic symptom disorder (DSM-5; under BDD Synonyms list in the core ICD-11)
Bodily distress disorder (core ICD-11; SNOMED CT)
Bodily Stress Syndrome (ICD-11 PHC guideline for 27 mental disorders)
Bodily distress syndrome (Fink et al 2010, operationalized in Denmark and beyond)plus the existing ICD-10 and SNOMED CT Somatoform disorders categories and their equivalents in ICPC-2.
5. A revised version of my report “Update on classification and coding of PVFS, ME and CFS for ICD-11” (v4 August 2020) is available to download
The PDF can be downloaded here.
Thumbnail pages 1 and 4:

6. The ICD-11 codes are now frozen
On February 10, 2020, the WHO stated on the Proposals platform: “The ICD-11 codes are now frozen. Proposed changes to the classification that would result in a code change are not permitted.”
Changes that would not disrupt the structure of the code hierarchies, for example, additions to the Index, addition or deletion of Synonym terms or Exclusion terms, edits to category Description texts or correction of typos are permissible.
But proposals for major changes such as relocating an existing Concept Title to a different chapter (which would necessitate a code change) or moving a term under a different “primary parent” code within its current chapter could not be considered.
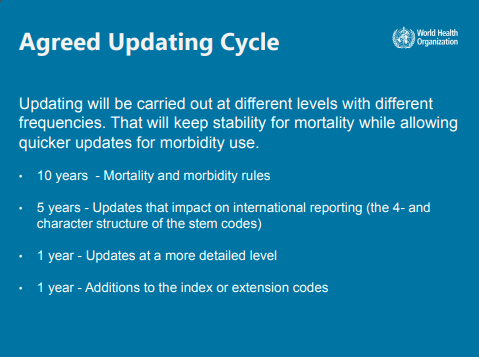
For further information on ICD-11 update schedules and what classes of changes are permitted see:
ICD-11 Reference Guide sections 3.8.1 to 2.8.7: 3.8 Annex: ICD-11 Updating and Maintenance






{kind=link}
{kind=link}
{kind=link}