ICD-11 Beta draft: Rationale for Proposal for Deletion of proposed new category: Bodily distress disorder
March 8, 2017
Post #328 Shortlink: http://wp.me/pKrrB-4dc
View on ICD-11 Proposal Mechanism: https://tinyurl.com/submissionDeleteBDD
(Registration with the Beta draft required in order to view proposals via the Beta draft Proposal Mechanism.)
PDF: ICD-11 Bodily distress disorder submission
Proposal submitted by Suzy Chapman (Dx Revision Watch) via ICD-11 Beta draft Proposal Mechanism
Submitted: March 1, 2017 (Remains unprocessed)
The author has no affiliations or conflicts of interest to declare.
Rationale for Proposal for Deletion of the Entity: Bodily distress disorder
1: The acronym “BDD” is already in use to indicate Body Dysmorphic Disorder [1].
2: With limited field studies, there is currently no substantial body of evidence for the validity, reliability, utility, prevalence, safety and acceptability of the S3DWG’s proposed disorder construct. However, the focus of this rationale is the proposed nomenclature.
The Somatic Distress and Dissociative Disorders Working Group (S3DWG) proposes to name its construct, “bodily distress disorder (BDD)” – a term that is already used by researchers and in the field interchangeably with the disorder term, “bodily distress syndrome (BDS).”
“Bodily distress syndrome” is a conceptually divergent disorder construct: differently defined and characterized, with different criteria that are already operationalized in Denmark and beyond, in research and clinical settings, and which potentially include a different patient set to that described in the S3DWG’s proposal [2].
As defined for the ICD-11 core version, the S3DWG’s “bodily distress disorder” construct has stronger conceptual and characterization alignment with DSM-5 “somatic symptom disorder (SSD)” than with Fink et al. (2010) “bodily distress syndrome” [3][4].
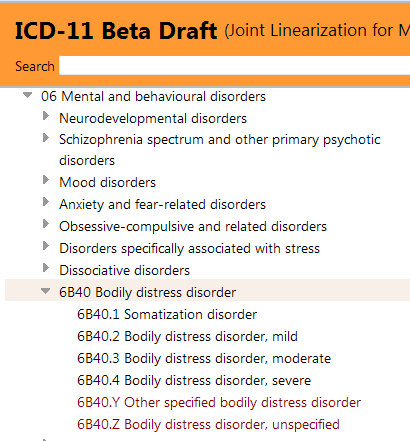
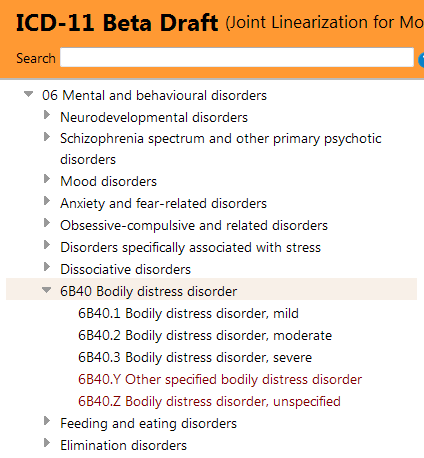
It is noted that “Somatic symptom disorder” is listed under Synonyms for the BDD entry in the ICD-11 Beta draft.
The defining feature of both the S3DWG’s “bodily distress disorder” and DSM-5 “somatic symptom disorder” is the removal of the distinction between “medically explained” and “medically unexplained” somatic complaints. Rather than define the disorder on the basis of the absence of a known medical cause, instead, specific psychological features are required in order to fulfill the criteria.
The S3DWG’s BDD is characterized by “the presence of bodily symptoms that are distressing to the individual and excessive attention directed toward the symptoms which may be manifest by repeated contact with health care providers.”
“Excessive attention is not alleviated by appropriate clinical examination and investigations and appropriate reassurance.”
“If a medical condition is causing or contributing to the symptoms, the degree of attention is clearly excessive in relation to its nature and progression.”
“Bodily symptoms and associated distress are persistent, being present on most days for at least several months and are associated with significant impairment in personal, family, social, educational, occupational or other important areas of functioning.”
The S3DWG’s “bodily distress disorder” may involve a single unspecified somatic symptom or multiple unspecified symptoms that may vary over time, in association with the disorder’s other defining features.
For DSM-5 “somatic symptom disorder,” the centrality of medically unexplained symptoms in order to meet the criteria is similarly de-emphasized and replaced by psychological responses to distressing, persistent symptoms: “excessive thoughts, behaviours and feelings” or “excessive preoccupation” with the bodily symptom or associated health concerns [5].
As with BDD, for SSD, the symptoms may or may not be associated with another medical condition. Some patients with general medical diagnoses, such as cancer, cardiovascular disease or diabetes, or patients diagnosed with the so-called “functional somatic syndromes” may qualify for a diagnosis of SSD if they are perceived as experiencing disproportionate and excessive thoughts and feelings or using maladaptive coping strategies in response to their illness, despite the reassurance of their clinicians [6].
As with the S3DWG’s defining of BDD, for SSD, there is no requirement for a specific number of complaints from among specified symptom groups to meet the criteria: so no symptoms counts or symptom clusters from body systems required for either.
To meet the SSD criteria: at least one symptom of at least six months duration and at least one of three psychological criteria are required: disproportionate thoughts about the seriousness of the symptom(s); or a high level of health anxiety; or devoting excessive time and energy to symptoms or health concerns; and for the symptoms to be significantly distressing or disruptive to daily life.
Though they differ somewhat in the characterization of their severity specifiers, the S3DWG’s defining of BDD and DSM-5 SSD may be considered essentially similar in conceptualization: no distinction between “medically explained” and “medically unexplained”; a much simplified criteria set to those defining the somatoform disorders, based on “excessive” or “disproportionate” psychological responses to persistent distressing symptoms, and with significant impairment or disruption to functioning.
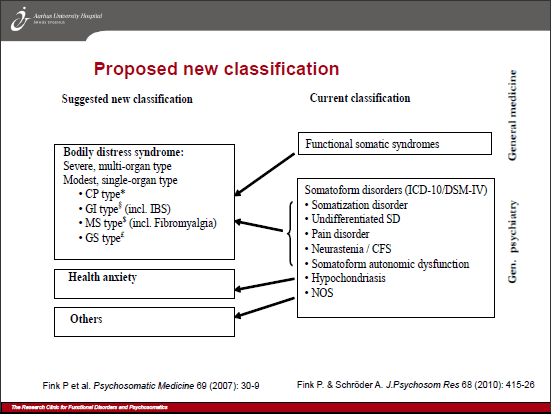
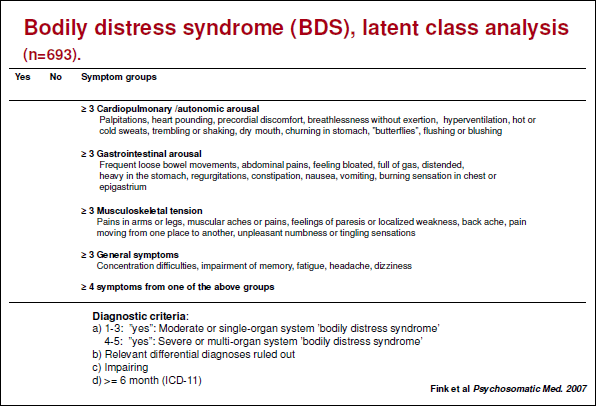
Whereas, for the Fink et al. (2010) “bodily distress syndrome (BDS),” psychological or behavioural characteristics are not part of the criteria: symptom patterns or clusters from organ/body systems (cardiopulmonary; gastrointestinal; musculoskeletal or general symptoms) are central [2]. The diagnosis is exclusively made on the basis of the somatic symptoms, their complexity and duration, with moderate to severe impairment of daily life. There is a “Moderate: single organ” type and a “Severe: multi-organ” type.
The Fink et al. (2010) BDS construct is considered by its authors to have the ability to capture the somatoform disorders, neurasthenia, “functional symptoms” and the so-called “functional somatic syndromes” under a single, unifying disorder construct which subsumes CFS, ME, fibromyalgia and IBS (which are discretely classified within other chapters of ICD-10), noncardiac chest pain, chronic pain disorder, MCS and some others [7][8][9].
(The various so-called specialty “functional somatic syndromes” are considered by the authors to be an artifact of medical specialization and manifestations of a similar, underlying disorder with a common, hypothesized aetiology.)
Contrast this with the S3DWG’s BDD construct, which makes no assumptions about aetiology and does not exclude symptoms associated with general medical conditions; whereas, for Fink et al. BDS, “If the symptoms are better explained by another disease, they cannot be labelled BDS.”
That DSM-5 SSD and Fink et al. (2010) BDS are differently conceptualized, with different criteria sets, potentially capturing different patient populations has been acknowledged by SSD work group chair, Joel E Dimsdale, and by Fink, Henningsen and Creed [10][11]. In the literature, however, one observes frequent instances where the term “bodily distress disorder” has been used when what is actually being discussed within the paper or editorial is the Fink et al. (2010) “bodily distress syndrome (BDS)” disorder construct.
For example, “bodily distress disorder” is used interchangeably with “bodily distress syndrome” in the editorial (Creed et al. 2010): Is there a better term than “medically unexplained symptoms”? [1].
In this (Rief and Isaac 2014) editorial: The future of somatoform disorders: somatic symptom disorder, bodily distress disorder or functional syndromes? the authors are using the term, “bodily distress disorder” while clearly discussing the Fink et al. (2010) BDS construct [12].
The S3DWG’s proposed term is seen, here, as “Bodily distress disorder (Fink and Schroder 2010)” in Slide #3 of the symposium presentation: An introduction to “medically unexplained” persistent physical symptoms. (Professor Trudie Chalder, Department of Psychological Medicine, King’s Health Partners, 2014) [13].
This recent paper: Medium- and long-term prognostic validity of competing classification proposals for the former somatoform disorders (Schumacher et al. 2017) compares prognostic validity of DSM-5 “somatic symptom disorder (SSD)” with “bodily distress disorder (BDD)” and “polysymptomatic distress disorder (PSDD)” and discusses their potential as alternatives to SSD for the replacement of the somatoform disorders for the forthcoming ICD-11 [14].
The authors state, “the current draft of the WHO group is based on the BDD proposal.” But the authors have confirmed that for their study, they had operationalized “Bodily distress disorder based on Fink et al. 2007” [15].
In the (Fink et al. 2007) paper: Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients, the authors conclude: “We identified a general, distinct, bodily distress syndrome or disorder that seems to encompass the various functional syndromes advanced by different medical specialties as well as somatization disorder and related diagnoses of the psychiatric classification.”
There are other examples in the literature and in the field. But these suffice to demonstrate that the term, “bodily distress disorder” is already used synonymously with disorder term “bodily distress syndrome (BDS)” and that researchers/clinicians, including Fink et al., do not differentiate between the two.
If researchers/clinicians do not differentiate between “bodily distress syndrome” and “bodily distress disorder” (and in some cases, one observes the conflations, “bodily distress syndrome or disorder” and “bodily distress syndrome/disorder”), has the S3DWG considered the difficulties and implications for maintaining the discrete identity of its proposed disorder, once ICD-11 is in the hands of its end users – clinicians, allied health professionals and coders; or considered the implications for patients and the particular vulnerability of those diagnosed with one of the so-called, “functional somatic syndromes”; or the implications for data reporting and analysis?
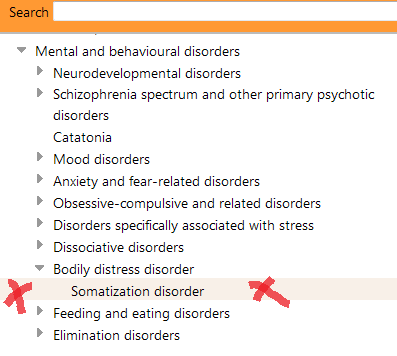
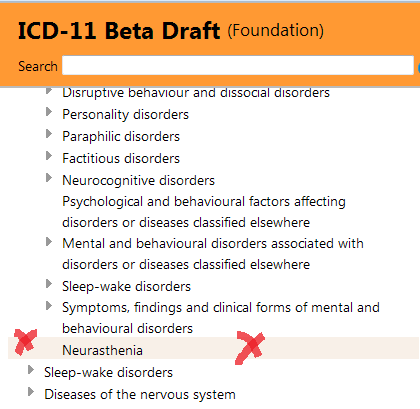
The S3DWG presented its emerging proposals for subsuming most of the ICD-10 somatoform disorder categories between F45.0 – F45.9, and F48.0 Neurasthenia, under a new single category which it proposes to call “bodily distress disorder (BDD)” in 2012 [3] and again in 2016 [4].
Thus far, the S3DWG has published no rationale for its recommendation to repurpose a disorder term already strongly associated with the Fink et al. (2010) disorder construct.
Neither has the group discussed nor acknowledged within its papers the implications for confusion and conflation between its own SSD- like “BDD” construct and the Fink et al. “bodily distress syndrome (BDS).”
Nor has the group’s output discussed the potential difficulties and implications for maintaining construct integrity within and beyond ICD-11.
There is no justification for introducing a new disorder category into ICD-11 that has greater conceptual alignment with the DSM-5 SSD construct but is proposed to be assigned a disorder name that is closely associated with a divergent (and operationalized) construct/criteria set, that is already in use in research and clinical settings.
This is unsafe and unsound classificatory practice.
This proposed disorder name should be rejected by the Project Lead for the revision of the Mental or behavioural disorders chapter and by the Joint Task Force that is overseeing the finalization of ICD-11 MMS.
If the S3DWG is unprepared or unwilling to reconsider and recommend an alternative disorder name then I submit that the current proposal to replace the somatoform disorders with a single “bodily distress disorder” category should be abandoned.
ICD-11 should proceed with the ICD-10 status quo, or retire or deprecate the somatoform disorder categories for the next edition.
It is perhaps germane that in 2010, three years prior to the finalization of DSM-5, Creed et al. had advanced: “Somatic symptom disorder is not a term that is likely to be embraced enthusiastically by doctors or patients; it has an uncertain core concept, dubious wide acceptability across cultures and does not promote multidisciplinary treatment. In our discussion, the terms which fit most closely the criteria we have set out above were the following: bodily distress (or stress) syndrome/ disorder, psychosomatic or psychophysical disorder, functional (somatic) syndrome or disorder.” [1]
The authors conclude that “bodily distress disorder” best fitted their “Criteria to judge the value of alternative terms for ‘medically unexplained symptoms.'”
It would appear that the term “bodily distress disorder” can mean anything anyone chooses it to mean – which might be admissible for Humpty Dumpty but unsound classificatory practice for ICD-11 [16].
References:
1 Creed F, Guthrie E, Fink P, Henningsen P, Rief W, Sharpe M, White P. Is there a better term than “medically unexplained symptoms”? J Psychosom Res. 2010 Jan;68(1):5-8. doi:10.1016/j.jpsychores.2009.09.004. [PMID: 20004295]
2 Fink P, Schröder A. One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders. J Psychosom Res. 2010 May;68(5):415-26. [PMID: 20403500]
3 Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry. 2012 Dec;24(6):556-67. doi: 10.3109/09540261.2012.741063. [PMID: 23244611]
4 Gureje O, Reed GM. Bodily distress disorder in ICD-11: problems and prospects. World Psychiatry. 2016 Oct;15(3):291-292. doi: 10.1002/wps.20353. [PMID: 27717252]
5 American Psychiatric Association. (2013). Somatic Symptom and Related Disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
6 Frances A, Chapman S. DSM-5 somatic symptom disorder mislabels medical illness as mental disorder. Aust N Z J Psychiatry. 2013 May;47(5):483-4. [PMID: 23653063]
7 Lam TP, Goldberg DP, Dowell AC, Fortes S, Mbatia JK, Minhas FA, Klinkman MS. Proposed new diagnoses of anxious depression and bodily stress syndrome in ICD-11-PHC: an international focus group study. Fam Pract. 2013 Feb;30(1):76-87. doi: 10.1093/fampra/cms037. Epub 2012 Jul 28. [PMID: 22843638]
8 Ivbijaro G, Goldberg D. Bodily distress syndrome (BDS): the evolution from medically unexplained symptoms (MUS). Ment Health Fam Med. 2013 Jun;10(2):63-4. [PMID: 24427171]
9 Goldberg DP, Reed GM, Robles R, Bobes J, Iglesias C, Fortes S, de Jesus Mari J, Lam TP, Minhas F, Razzaque B et al. Multiple somatic symptoms in primary care: A field study for ICD-11 PHC, WHO’s revised classification of mental disorders in primary care settings. J Psychosom Res. 2016 Dec;91:48-54. doi:10.1016/j.jpsychores.2016.10.002. Epub 2016 Oct 4. [PMID: 27894462]
10 Medically Unexplained Symptoms, Somatisation and Bodily Distress: Developing Better Clinical Services, Francis Creed, Peter Henningsen, Per Fink (Eds), Cambridge University Press, 2011.
11 Frances Creed and Per Fink. Presentations, Research Clinic for Functional Disorders Symposium, Aarhus University Hospital, May 15, 2014.
12 Rief W, Isaac M. The future of somatoform disorders: somatic symptom disorder, bodily distress disorder or functional syndromes? Curr Opin Psychiatry September 2014 – Volume 27 – Issue 5 – p315–319. [PMID: 25023885]
13 Chalder, T. An introduction to “medically unexplained” persistent physical symptoms. Presentation, Department of Psychological Medicine, King’s Health Partners, 2014. [Accessed 27 February 2017]
14 Schumacher S, Rief W, Klaus K, Brähler E, Mewes R. Medium- and long-term prognostic validity of competing classification proposals for the former somatoform disorders. Psychol Med. 2017 Feb 9:1-14. doi: 10.1017/S0033291717000149. [PMID: 28179046]
15 Fink P, Toft T, Hansen MS, Ornbol E, Olesen F. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients. Psychosom Med. 2007 Jan;69(1):30-9. [PMID: 17244846]
16 Carroll L. Alice’s Adventures in Wonderland. 1885. Macmillan.





{kind=link}
{kind=link}
{kind=link}