Global creep of DSM-5’s Somatic symptom disorder
March 25, 2014
Post #303 Shortlink: http://wp.me/pKrrB-3Qq
Update at April 14, 2014:
Written response (April 10, 2014) from Independent Hospital Pricing Authority (IHPA) to request for clarification regarding the term ‘Somatic symptom disorder’ and Australia’s clinical modification of ICD-10, ICD-10-AM:
PDF: IHPA response re SSD and ICD-10-AM
As previously posted:
In the previous posting Update on proposal to add DSM-5′s Somatic symptom disorder to ICD-10-CM I reported that NCHS is preparing to rubber stamp proposals to insert Somatic symptom disorder into the U.S.’s forthcoming clinical modification of ICD-10.
Comments/objections to Diagnosis Agenda proposals submitted at the March meeting need to be sent by email to NCHS at nchsicd9CM@cdc.gov by June 20th.
1] According to this Australian legislative document:
http://www.comlaw.gov.au/Details/F2014L00304
Australian Government, Statement of Principles concerning somatic symptom disorder No. 24 of 2014
for the purposes of the Veterans’ Entitlements Act 1986 and Military Rehabilitation and Compensation Act 2004
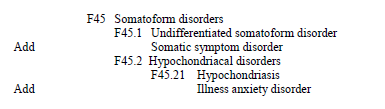
“Somatic symptom disorder attracts ICD-10-AM code F45.1.”
For the purposes of the Statement of Principles:
“ICD-10-AM code” means a number assigned to a particular kind of injury or disease in The International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM), Eighth Edition, effective date of 1 July 2013, copyrighted by the Independent Hospital Pricing Authority, and having ISBN 978-1-74128-213-9;”
The Australian ICD-10-CM, Eighth Edition, July 2013 is not in the public domain. As I do not have access to a copy, I have contacted the relevant body for clarifications.
I have asked whether Somatic symptom disorder has been added to the Eighth Edition of ICD-10-AM as an Inclusion term to F45.1 Undifferentiated somatoform disorder in the Tabular List and Alphabetical Index.
Or, whether this legislative document relies on the ICD cross-walk codes as published in the DSM-5 in May 2013 for the cross-walk between DSM-5 disorders and the disorders in the U.S.’s ICD-9-CM and forthcoming ICD-10-CM.
Or, whether the legislative document relies on a cross-walk between DSM-5 disorders and ICD-10-AM codes developed specifically in relation to the ICD-10-AM Eighth Edition, July 2013.
I will update this post when I have received clarification.
According to this page: http://nccc.uow.edu.au/icd10am-achi-acs/overview/icd10am/index.html
“[Australia’s] ICD-10-AM has also enjoyed more widespread use, having been assessed, found suitable and adopted by many other countries, including: New Zealand, Ireland, Singapore, Slovenia.”
I am unable to confirm how many countries that have adopted ICD-10-AM have migrated from earlier editions to the July 2013 edition or are preparing to migrate to the most recent edition.
Other clinical modifications (CMs) of ICD-10:
Canada (ICD-10-CA): The most recent edition of ICD-10-CA is the 2009 edition Volume One: Tabular List 2009. Canada is anticipated to adopt a CM of ICD-11 before the U.S. does, but in meantime, an updated edition of ICD-10-CA might be anticipated, especially given the recent extension to the ICD-11 development timeline. Canadians will need to be alert to the potential for addition of SSD as an inclusion term to the next edition of ICD-10-CA.
Germany (ICD-10-GM): There is an ICD-10-GM version for 2014. There is no SSD under F45.x or under any other code, but watch for any updated versions released prior to transition to a CM of ICD-11.
Thailand (ICD-10-TM): There does not appear to be a more recent version of the Thai clinical modification than the online version for 2007, but watch for SSD in any updated versions prior to potential transition to a CM of ICD-11. ICD-10-TM Online version for 2007.
ICD-11 Beta drafting platform:
There is no documentary evidence of a proposal to add SSD, per se, to ICD-11. However, the wording for the Definition for Bodily distress disorder, as it currently stands in the Beta drafting platform, is drawn from the Gureje, Creed 2012 paper on the S3DWG sub working group’s emerging proposals for ICD-11 [1].
The paper described a simplified disorder framework – a construct into which DSM-5′s Somatic Symptom Disorder could be comfortably integrated, thus facilitating harmonization between the respective ICD-11 and DSM-5 disorder construct and criteria replacements for the Somatoform disorders classifications.
As with DSM-5′s SSD, for the emerging proposals for BDD, the focus was not on symptoms counts, or on strict symptom patterns or clusters from one or more body systems, or on whether symptoms were determined as being “medically explained” or “medically unexplained,” but on the perception of disproportionate or maladaptive psychobehavioural responses to, or excessive preoccupation with any troublesome chronic bodily symptom(s). And that in doing away with the “unreliable assumption of its causality” the diagnosis of BDD would not exclude the presence of a co-occurring physical health condition – which is very close to SSD’s defining characteristics.
1. Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry. 2012 Dec;24(6):556-67. http://www.ncbi.nlm.nih.gov/pubmed/23244611 [Abstract. Full text behind paywall]
2] On the Patient.co.uk site, a peer reviewed article on Somatic symptom disorder:
http://www.patient.co.uk/doctor/somatic-symptom-disorder
This article is not a recommendation and it draws heavily on the DSM-IV and current ICD-10 Somatoform disorders framework, criteria and literature. Though it does highlight that DSM-5 has a new, simplified framework and reformulated criteria that rely less on strict patterns of somatic symptoms and more on the degree to which a patient’s thoughts, feelings and behaviours about their symptoms are considered disproportionate or excessive; that for DSM-5, “medically unexplained” is de-emphasized – symptoms may or may not be associated with another medical condition and patients with organic comorbidities such as heart disease, osteoarthritis or cancer, who would have previously been excluded under DSM-IV, can now be included in the diagnosis of SSD.
There is little published research examining the reliability, utility, epidemiology, clinical characteristics or treatment of Somatic symptom disorder as a diagnostic construct and none of the article’s references are for papers specifically using the new Somatic symptom disorder criteria.
3] Somatic symptom disorder in a BMJ Rapid Response:
Rapid Response to: Clinical Review, Fibromyalgia by Anisur Rahman, Martin Underwood, Dawn Carnes [Full text for Clinical Review behind paywall]
http://www.bmj.com/content/348/bmj.g1224/rr/689294
Rapid Response: Fibromyalgia: an unhelpful diagnosis for both patients and doctors [Full text for Rapid Response accessible]
Christopher Bass, consultant in liaison psychiatry, John Radcliffe Hospital , Oxford OX3 9DU
Dr Max Henderson, senior lecturer in Epidemiology and Occupational psychiatry, Inststitute of psychiatry, Kings College London
According to the authors, fibromyalgia ( coded in ICD-10 under Chapter XXIII Diseases of the musculoskeletal system and connective tissue, at M79.7 ) is more appropriately described in terms of “polysymptomatic distress”; “polysymptomatic distress has been recognised as a somatoform disorder, specifically as a somatic symptom disorder or SSD,” and that since “FM overlaps with other disorders with medically unexplained symptoms such as irritable bowel syndrome and chronic fatigue syndrome” it is more appropriate to treat them with multidisciplinary teams within the same specialised service in the general hospital.
4] This commentary by infectious disease specialist, Judy Stone, MD, at Scientific American blogs, mentions concerns around SSD:
Have Pain? Are You Crazy? Rare Diseases Pt. 2
By Judy Stone | February 18, 2014
“It’s all in your head,” patients with unexplained pain or unexpected symptoms often hear…
5] Halifax Somatic Symptoms Disorder Trial
http://clinicaltrials.gov/show/NCT02076867
ClinicalTrials.gov Identifier: NCT02076867
Sponsor: Capital District Health Authority, Canada
The purpose of this study is to compare the effectiveness of Intensive Short-Term Dynamic Psychotherapy (ISTDP) plus Medical Care As Usual (MCAU) compared to MCAU for Somatic Symptom and Related Disorders (SSRD). Consenting patients presenting to the emergency department with suspected SSRD will be randomly allocated to receive either 8 weekly individual sessions of ISTDP or to an 8-week wait list followed by ISTDP. MCAU including emergency department and/or family doctor consultation is available throughout trial participation. The primary outcome measure is participant self-reported somatic symptoms at week 8.


Next meeting of ICD-10-CM Coordination and Maintenance Committee is March 19-20, 2014
November 16, 2013 by admindxrw
Post #282 Shortlink: http://wp.me/pKrrB-3xE
The deadline for receipt of public submissions in response to proposals for updates and changes to ICD-10-CM diagnosis and procedure codes presented at the September 18-19, 2013 meeting of the ICD-9-CM Coordination and Maintenance Committee has now closed.
In 2014, this advisory Committee, which is co-chaired by NCHS and CMS, will be known as the ICD-10-CM Coordination and Maintenance Committee, as there will be no further updates of ICD-9-CM.
A done deal?
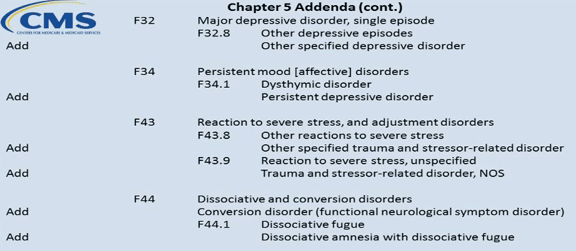
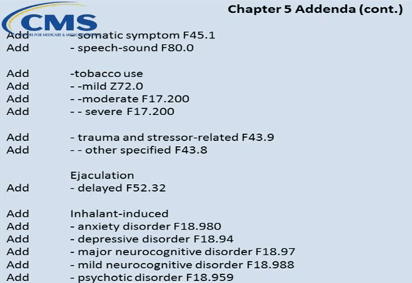
Proposals submitted on behalf of the American Psychiatric Association (APA) and presented at the meeting by APA’s Research Director, Darrel Regier, MD, can be found from Page 32 of the Diagnosis Agenda. Additional proposals for inclusion of new DSM-5 disorder terms within ICD-10-CM Chapter 5 Mental and behavioral disorders can be found on Pages 45-46.
The Summary of the September meeting diagnosis presentations can be found here. Links for the four videocasts of the meeting’s two day proceedings are listed in this Dx Revision Watch post and the Meeting Materials are here.
The Timeline for ICD-9-CM (for the remainder of its life) and for ICD-10-CM is set out from Page 3 of the Diagnosis Agenda.
Some diagnosis proposals at the September 18-19, 2013 meeting were requested for October 2014 implementation and some for 2015 implementation. I shall update this site when the outcomes of the various proposals are published, next year.
There is a lack of clarity over which body has requested the addition of Somatic symptom disorder (SSD) and Illness anxiety disorder as inclusion terms to existing ICD-10-CM codes. It isn’t clear whether these two additional DSM-5 constructs have been proposed for inclusion in ICD-10-CM by the APA or by the NCHS/CMS Committee – if the latter, should we assume these two proposals already have the support of NCHS?
Given APA’s determination to achieve harmonization between the two systems, the outcome of its proposals to insert a handful of new DSM-5 disorders into ICD-10-CM may already be a done deal between APA and NCHS: the Director of NCHS may not need much persuasion to ratify their retrofitting into ICD-10-CM.
Loss of public trust and confidence
If NCHS is planning to rubber stamp insertion into ICD-10-CM of DSM-5’s poorly validated Somatic symptom disorder in response to APA diktat, having conducted no field testing and in the absence of a body of supportive evidence for SSD’s clinical relevance, safety and utility, and with disregard for a high level of public concern, what confidence can the public have that this federal agency is meeting its duty of care towards patient populations and towards the clinicians and allied health professionals who may deploy this proposed new ICD term, in its ethics, integrity and methods and for upholding standards of scientific rigour?
APA may re-present proposals next year
If APA is unsuccessful with any of the additions requested via the September meeting, it is possible that the organization may re-present proposals or modified proposals at the next C & M Committee meeting, scheduled for March 19-20, 2014. There are also other new DSM-5 disorders or changes that APA might potentially propose for incorporation into ICD-10-CM at the March 2014 or the September 2014 meeting, or at some later point.
Only a brief public submission period for March 2014 meeting
March 19-20, 2014 meeting
The deadline for Requestors to submit proposals for consideration for the March meeting agenda is January 17, 2014.
The draft agenda will be posted in February 2014.
Registration is required for those wishing to attend the meeting. Register online between on February 14 – March 14.
The two day meeting is scheduled for March 19 – 20.
Note: the deadline for receipt of comments on the March 19-20, 2014 meeting proposals for both procedure and diagnosis codes and changes is given as April 18. So instead of a couple of months for stakeholder responses, it appears there will only be four weeks or so in which to prepare and submit comments or objections.
I will post the Diagnosis Agenda for the March 2014 meeting as soon as it becomes available and links for the videocasts of the proceedings after the meeting has taken place. (Videocasts now substitute for written transcripts of meeting proceedings.)
Extracts from the Timeline that relate to the publication of additions and changes for ICD-10-CM:
April 2014 Notice of Proposed Rulemaking to be published in the Federal Register as mandated by Public Law 99-509. This notice will include references to the complete and finalized FY 2015 ICD-10-CM diagnosis and ICD-10-PCS procedure codes. It will also include proposed revisions to the MS-DRG system based on ICD-10-CM/PCS codes on which the public may comment. The proposed rule can be accessed here.
June 2014 Final addendum posted on web pages as follows:
Diagnosis addendum – http://www.cdc.gov/nchs/icd/icd10cm.htm
Procedure addendum – http://cms.hhs.gov/Medicare/Coding/ICD10/index.html
October 1, 2014 New and revised ICD-10-CM and ICD-10-PCS codes go into effect along with DRG changes. Final addendum posted on web pages as follows:
Diagnosis addendum – http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
Procedure addendum – http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/addendum.html
November 2014 Any new ICD-10 codes required to capture new technology that will be implemented on the following April 1 will be announced. Information on any new codes to be implemented April 1, 2015 will be posted on the following websites:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/addendum.html
http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
Share this:
Filed under American Psychiatric Association (APA), Darrel Regier, Diagnostic classification, DSM-5, ICD-10-CM, ICD-11, MUS, Somatic Symptom Disorder, Somatoform Disorders, WHO Collaborating Centre Tagged with american psychiatric association, dsm-5, icd-10-cm, icd-11, illness anxiety disorder, institute of psychiatry, NCHS, public comment, somatic symptom disorder, somatoform disorders