[PDF] DEPARTMENT OF HEALTH AND HUMAN SERVICES, Office of the Secretary
45 CFR Part 162 [CMS-0043-F] RIN 0938-AS31
Administrative Simplification: Change to the Compliance Date for the International Classification of Diseases, 10th Revision (ICD–10–CM and ICD-10-PCS) Medical Data Code Sets
Deadline for ICD-10 allows health care industry ample time to prepare for change
Deadline set for October 1, 2015
The U.S. Department of Health and Human Services (HHS) issued a rule today finalizing Oct. 1, 2015 as the new compliance date for health care providers, health plans, and health care clearinghouses to transition to ICD-10, the tenth revision of the International Classification of Diseases. This deadline allows providers, insurance companies and others in the health care industry time to ramp up their operations to ensure their systems and business processes are ready to go on Oct. 1, 2015.
The ICD-10 codes on a claim are used to classify diagnoses and procedures on claims submitted to Medicare and private insurance payers. By enabling more detailed patient history coding, ICD-10 can help to better coordinate a patient’s care across providers and over time. ICD-10 improves quality measurement and reporting, facilitates the detection and prevention of fraud, waste, and abuse, and leads to greater accuracy of reimbursement for medical services. The code set’s granularity will improve data capture and analytics of public health surveillance and reporting, national quality reporting, research and data analysis, and provide detailed data to enhance health care delivery. Health care providers and specialty groups in the United States provided extensive input into the development of ICD-10, which includes more detailed codes for the conditions they treat and reflects advances in medicine and medical technology.
“ICD-10 codes will provide better support for patient care, and improve disease management, quality measurement and analytics,” said Marilyn Tavenner, Administrator of the Centers for Medicare & Medicaid Services (CMS). “For patients under the care of multiple providers, ICD-10 can help promote care coordination.”
Using ICD-10, doctors can capture much more information, meaning they can better understand important details about the patient’s health than with ICD-9-CM. Moreover, the level of detail that is provided for by ICD-10 means researchers and public health officials can better track diseases and health outcomes. ICD-10 reflects improved diagnosis of chronic illness and identifies underlying causes, complications of disease, and conditions that contribute to the complexity of a disease. Additionally, ICD-10 captures the severity and stage of diseases such as chronic kidney disease, diabetes, and asthma.
The previous revision, ICD-9-CM, contains outdated, obsolete terms that are inconsistent with current medical practice, new technology and preventive services.
ICD-10 represents a significant change that impacts the entire health care community. As such, much of the industry has already invested resources toward the implementation of ICD-10. CMS has implemented a comprehensive testing approach, including end-to-end testing in 2015, to help ensure providers are ready. While many providers, including physicians, hospitals, and health plans, have completed the necessary system changes to transition to ICD-10, the time offered by Congress and this rule ensure all providers are ready.
This report updates on the revised implementation date for ICD-10-CM, the revised Partial Code Freeze timeline, the ICD-10-CM Release for 2015 files, and a reminder of the deadline for objections to the insertion of DSM-5’s Somatic symptom disorder into ICD-10-CM.
[For reminder of deadline for objections to proposed insertion of Somatic symptom disorder into ICD-10-CM, skip to red subheading.]
On April 1, 2014, Bill H.R. 4302, known as the PAM Act (Protecting Access to Medicare Act), was signed into law by President Obama.
As a result of a quietly inserted clause piggybacking on this Bill, implementation of ICD-10-CM was delayed by a further year. Centers for Medicare & Medicaid Services (CMS) has confirmed that the effective implementation date for ICD-10-CM is now October 1, 2015.
Until that time, the codes in ICD-10-CM (the U.S. specific adaptation of the WHO’s ICD-10) are not valid for any purpose or use.
+++
Partial Code Freeze
CMS has announced that the partial code freeze on updates to the ICD-9-CM and ICD-10-CM diagnosis and procedure codes will continue until October 1, 2015.
Between October 1, 2011 and October 1, 2016 revisions to ICD-10-CM/PCS will be for new diseases/new technology procedures, and any minor revisions to correct reported errors in these classifications. Regular (at least annual) updates to ICD-10-CM/PCS will resume on October 1, 2016.
The ICD-10 Coordination and Maintenance Committee (formerly the ICD-9-CM Coordination and Maintenance Committee) implemented a partial freeze of the ICD-9-CM and ICD-10 (ICD-10-CM and ICD-10-PCS) codes prior to the implementation of ICD-10 which would end one year after the implementation of ICD-10. There was considerable support for this partial freeze. On April 1, 2014, the Protecting Access to Medicare Act of 2014 (PAMA) (Pub. L. No. 113-93) was enacted, which said that the Secretary may not adopt ICD-10 prior to October 1, 2015. Accordingly, the U.S. Department of Health and Human Services expects to release an interim final rule in the near future that will include a new compliance date that would require the use of ICD-10 beginning October 1, 2015. The rule will also require HIPAA covered entities to continue to use ICD-9-CM through September 30, 2015. When published, links will be provided to this interim final rule at http://www.cms.gov/Medicare/Coding/ICD10/Statute_Regulations.html
The partial freeze will be implemented as follows:
• The last regular, annual updates to both ICD-9-CM and ICD-10 code sets were made on October 1, 2011.
• On October 1, 2012, October 1, 2013, and October 1, 2014 there will be only limited code updates to both the ICD-9-CM and ICD-10 code sets to capture new technologies and diseases as required by section 503(a) of Pub. L. 108-173.
• On October 1, 2015, there will be only limited code updates to ICD-10 code sets to capture new technologies and diagnoses as required by section 503(a) of Pub. L. 108-173. There will be no updates to ICD-9-CM, as it will no longer be used for reporting.
• On October 1, 2016 (one year after implementation of ICD-10), regular updates to ICD-10 will begin.
The ICD-10 Coordination and Maintenance Committee will continue to meet twice a year during the partial freeze. At these meetings, the public will be asked to comment on whether or not requests for new diagnosis or procedure codes should be created based on the criteria of the need to capture a new technology or disease. Any code requests that do not meet the criteria will be evaluated for implementation within ICD-10 on and after October 1, 2016 once the partial freeze has ended.
CDC has not yet updated its webpages to reflect the ICD-10-CM implementation delay or the revised Partial Code Freeze timeline.
+++
SSD and ICD-10-CM/PCS Coordination and Maintenance Committee proposals
At the September 2013 and March 2014 Coordination and Maintenance Committee meetings, the American Psychiatric Association (APA) submitted numerous requests for addenda changes for new index entries and tabular inclusion terms for evaluation for implementation on October 1, 2015.
It is unclear whether requests for modifications submitted by APA and other requestors via these September and March meetings will be rolled forward for evaluation for implementation on and after the revised date of October 1, 2016 or whether these proposals will now need to be resubmitted at future C & M Committee meetings. (The next public meeting takes place September 23–24, 2014.)
I have approached NCHS for clarification.
+++
If the proposals from these two meetings do require resubmitting, this would provide another opportunity to comment on the proposal to add the DSM-5’s new disorder term, Somatic symptom disorder, to the ICD-10-CM.
+++
At the public Coordination and Maintenance Committee meeting on September 18–19, 2013, a proposal had been submitted to add Somatic symptom disorder (SSD) as an inclusion term to existing ICD-10-CM code F45.1 Undifferentiated somatoform disorder in the Tabular List Addendum (this also included addition to the Index).
Note: Proposal is not to create a unique code for SSD or to replace any of the existing ICD-10-CM somatoform disorders with SSD, but to add SSD as an inclusion term under an existing ICD-10-CM code, F45.1.
September 18–19, 2013 meeting Agenda, Page 45: PDF Agenda
+++
The proposal to add somatic symptom disorder to the Index (under Disorder), was resubmitted at the public meeting on March 19–20, (reason unclear but a number of proposals for modifications to both the Tabular List and the Index from the September 2013 meeting were also duplicated at the March 2014 meeting).
March 19–20, 2014 meeting Agenda, Page 89: PDF Agenda
+++
Any decisions made on the considerable number of proposals requested at last year’s September meeting are yet to be posted and possibly won’t be evident until the relevant Addendum is released.
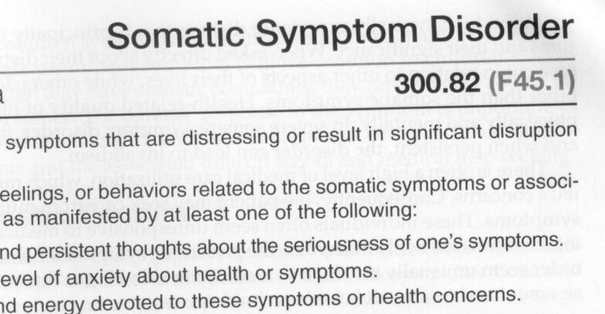
In the DSM-5, Somatic symptom disorder is already cross-walked to ICD-9 code 300.82 (ICD-10-CM F45.1):
+++ DSM-5 (Page 311)
+++
Given that APA worked with CDC on the cross-walk between the new DSM-5 disorder terms and ICD-9/ICD-10-CM equivalent codes, NCHS’s Director will likely rubber stamp the APA’s proposals for insertion of SSD and a number of other new DSM-5 categories.
Nevertheless, I shall be putting in another objection before the June 20 deadline and I hope all stakeholders with concerns will strongly oppose the incorporation of this controversial new disorder construct into ICD-10-CM.
The deadline for comments on proposals requested at the March meeting is June 20th.
Send comments, by email, to NCHS to nchsicd9CM@cdc.gov
+++ Not a small thing
Between 2010 and 2012, the SSD Work Group attracted considerable opposition across three stakeholder reviews to its radical proposals for a replacement for the somatoform disorders.
In late 2012 and early 2013, we saw a good deal of “outrage” in comments to articles by Allen Frances and myself here and here at Psychology Today and here in the BMJ, in response to the cavalier decision by the Task Force to barrel through with the SSD Work Group’s poorly validated disorder construct.
But I see little evidence of sustained opposition from U.S. professionals and patients over the September and March NCHS/CMS update and revision meeting proposals to insinuate SSD into ICD-10-CM.
At the moment, the proposal is for inserting SSD as an inclusion term under an existing category – not to create a unique code for SSD and not to replace the existing framework with SSD. At the September meeting, CDC’s Donna Pickett said:
“…And just to complete the package, there are other Tabular List proposals that appear on Page 45 and 46 that we would also invite your comments on. And again, with some of the terminology changes that Dr Regier has described the intent here is to make sure that if those terms are being used, that they do have a home somewhere within ICD-10-CM to facilitate people looking these up. So we invite comments…”
Sounds almost cosy. But if NCHS does rubber stamp the addition of Somatic symptom disorder to ICD-10-CM, it could leverage future replacement of the existing Somatoform disorders categories with this new, single diagnostic construct, bringing ICD-10-CM’s framework in line with DSM-5.
There are implications for ICD-11, too.
Once SSD is inserted into ICD-10-CM, the presence of this term within the U.S. modification of ICD-10 may make it easier for ICD-11 Revision Steering Group to justify approving proposals to replace the existing ICD-10 Somatoform disorders categories with a single, new disorder construct that would mirror SSD’s defining characteristics – its positive psychobehavioural features, its simplified criteria, its de-emphasis on “medically unexplained” – and facilitate harmonization between ICD-11 and DSM-5 disorder terms.
Christopher Chute, Mayo, chairs the ICD-11 Revision Steering Group. Chute has suggested that following implementation, ICD-10-CM might be brought gradually in line with ICD-11 through a series of annual updates, for smoother transition to ICD-11-CM.
Inserting the SSD term into ICD-10-CM paves the way for disorder construct congruency between DSM-5, ICD-10-CM, ICD-11, and eventually, the ICD-11-CM modification.
Send comments, by email, by June 20, to NCHS at nchsicd9CM@cdc.gov
CMS posts files for ICD-10-CM Release for 2015
On May 15, CMS posted the ICD-10 Procedure Coding System (ICD-10-PCS) files for 2015, download files here:
These files (some of which are large ZIP files) include:
2015 Code Descriptions in Tabular Order
2015 Code Tables and Index – Updated 5/22/14 (includes Tabular List, and Index in PDF format)
2015 ICD-10-CM Duplicate Code Numbers
2015 Addendum
2015 General Equivalence Mappings (GEMs) – Diagnosis Codes and Guide
2015 Reimbursement Mappings – Diagnosis Codes and Guide
According to the Addendum, “There were no changes to the 2014 ICD-10-CM, therefore there are no 2015 ICD-10-CM Addenda.”
These ICD-10-CM Release for 2015 files are not yet available on the CDC site but when they are posted, they should be accessible from this page: http://www.cdc.gov/nchs/icd/icd10cm.htm
Written response (April 10, 2014) from Independent Hospital Pricing Authority (IHPA) to request for clarification regarding the term ‘Somatic symptom disorder’ and Australia’s clinical modification of ICD-10, ICD-10-AM:
“ICD-10-AM code” means a number assigned to a particular kind of injury or disease in The International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM), Eighth Edition, effective date of 1 July 2013, copyrighted by the Independent Hospital Pricing Authority, and having ISBN 978-1-74128-213-9;”
The Australian ICD-10-CM, Eighth Edition, July 2013 is not in the public domain. As I do not have access to a copy, I have contacted the relevant body for clarifications.
I have asked whether Somatic symptom disorder has been added to the Eighth Edition of ICD-10-AM as an Inclusion term to F45.1 Undifferentiated somatoform disorder in the Tabular List and Alphabetical Index.
Or, whether this legislative document relies on the ICD cross-walk codes as published in the DSM-5 in May 2013 for the cross-walk between DSM-5 disorders and the disorders in the U.S.’s ICD-9-CM and forthcoming ICD-10-CM.
Or, whether the legislative document relies on a cross-walk between DSM-5 disorders and ICD-10-AM codes developed specifically in relation to the ICD-10-AM Eighth Edition, July 2013.
I will update this post when I have received clarification.
“[Australia’s] ICD-10-AM has also enjoyed more widespread use, having been assessed, found suitable and adopted by many other countries, including: New Zealand, Ireland, Singapore, Slovenia.”
I am unable to confirm how many countries that have adopted ICD-10-AM have migrated from earlier editions to the July 2013 edition or are preparing to migrate to the most recent edition.
Other clinical modifications (CMs) of ICD-10:
Canada (ICD-10-CA): The most recent edition of ICD-10-CA is the 2009 edition Volume One: Tabular List 2009. Canada is anticipated to adopt a CM of ICD-11 before the U.S. does, but in meantime, an updated edition of ICD-10-CA might be anticipated, especially given the recent extension to the ICD-11 development timeline. Canadians will need to be alert to the potential for addition of SSD as an inclusion term to the next edition of ICD-10-CA.
Germany (ICD-10-GM): There is an ICD-10-GM version for 2014. There is no SSD under F45.x or under any other code, but watch for any updated versions released prior to transition to a CM of ICD-11.
Thailand (ICD-10-TM): There does not appear to be a more recent version of the Thai clinical modification than the online version for 2007, but watch for SSD in any updated versions prior to potential transition to a CM of ICD-11. ICD-10-TM Online version for 2007.
ICD-11 Beta drafting platform:
There is no documentary evidence of a proposal to add SSD, per se, to ICD-11. However, the wording for the Definition for Bodily distress disorder, as it currently stands in the Beta drafting platform, is drawn from the Gureje, Creed 2012 paper on the S3DWG sub working group’s emerging proposals for ICD-11 [1].
The paper described a simplified disorder framework – a construct into which DSM-5′s Somatic Symptom Disorder could be comfortably integrated, thus facilitating harmonization between the respective ICD-11 and DSM-5 disorder construct and criteria replacements for the Somatoform disorders classifications.
As with DSM-5′s SSD, for the emerging proposals for BDD, the focus was not on symptoms counts, or on strict symptom patterns or clusters from one or more body systems, or on whether symptoms were determined as being “medically explained” or “medically unexplained,” but on the perception of disproportionate or maladaptive psychobehavioural responses to, or excessive preoccupation with any troublesome chronic bodily symptom(s). And that in doing away with the “unreliable assumption of its causality” the diagnosis of BDD would not exclude the presence of a co-occurring physical health condition – which is very close to SSD’s defining characteristics.
1. Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry. 2012 Dec;24(6):556-67. http://www.ncbi.nlm.nih.gov/pubmed/23244611 [Abstract. Full text behind paywall]
2] On the Patient.co.uk site, a peer reviewed article on Somatic symptom disorder:
This article is not a recommendation and it draws heavily on the DSM-IV and current ICD-10 Somatoform disorders framework, criteria and literature. Though it does highlight that DSM-5 has a new, simplified framework and reformulated criteria that rely less on strict patterns of somatic symptoms and more on the degree to which a patient’s thoughts, feelings and behaviours about their symptoms are considered disproportionate or excessive; that for DSM-5, “medically unexplained” is de-emphasized – symptoms may or may not be associated with another medical condition and patients with organic comorbidities such as heart disease, osteoarthritis or cancer, who would have previously been excluded under DSM-IV, can now be included in the diagnosis of SSD.
There is little published research examining the reliability, utility, epidemiology, clinical characteristics or treatment of Somatic symptom disorder as a diagnostic construct and none of the article’s references are for papers specifically using the new Somatic symptom disorder criteria.
3] Somatic symptom disorder in a BMJ Rapid Response:
Rapid Response to: Clinical Review, Fibromyalgia by Anisur Rahman, Martin Underwood, Dawn Carnes [Full text for Clinical Review behind paywall]
Rapid Response: Fibromyalgia: an unhelpful diagnosis for both patients and doctors [Full text for Rapid Response accessible]
Christopher Bass, consultant in liaison psychiatry, John Radcliffe Hospital , Oxford OX3 9DU
Dr Max Henderson, senior lecturer in Epidemiology and Occupational psychiatry, Inststitute of psychiatry, Kings College London
According to the authors, fibromyalgia ( coded in ICD-10 under Chapter XXIII Diseases of the musculoskeletal system and connective tissue, at M79.7 ) is more appropriately described in terms of “polysymptomatic distress”; “polysymptomatic distress has been recognised as a somatoform disorder, specifically as a somatic symptom disorder or SSD,” and that since “FM overlaps with other disorders with medically unexplained symptoms such as irritable bowel syndrome and chronic fatigue syndrome” it is more appropriate to treat them with multidisciplinary teams within the same specialised service in the general hospital.
4] This commentary by infectious disease specialist, Judy Stone, MD, at Scientific American blogs, mentions concerns around SSD:
Sponsor: Capital District Health Authority, Canada
The purpose of this study is to compare the effectiveness of Intensive Short-Term Dynamic Psychotherapy (ISTDP) plus Medical Care As Usual (MCAU) compared to MCAU for Somatic Symptom and Related Disorders (SSRD). Consenting patients presenting to the emergency department with suspected SSRD will be randomly allocated to receive either 8 weekly individual sessions of ISTDP or to an 8-week wait list followed by ISTDP. MCAU including emergency department and/or family doctor consultation is available throughout trial participation. The primary outcome measure is participant self-reported somatic symptoms at week 8.
Update at April 5, 2014: Implementation of the U.S.’s forthcoming adaptation of ICD-10, ICD-10-CM, has been kicked further down the road to no earlier than October 1, 2015.
Bill H.R. 4302, known as the PAM Act (Protecting Access to Medicare Act), was signed into law by President Obama on April 1, 2014. This means that the U.S. cannot now transition from ICD-9-CM to ICD-10-CM on October 1, 2014. CMS has yet to issue a full statement, update its webpages and issue guidelines for a new implementation date. No statement has yet been made concerning the impact of this legislation on the timeline for the ICD-10-CM update process during a partial code freeze.
Lots of “outrage” over SSD and DSM-5 but I see little evidence of sustained “outrage” over proposals to add SSD as an Inclusion term to the U.S.’s ICD-10-CM.
If NCHS rubber stamps the addition of Somatic Symptom Disorder to ICD-10-CM it could leverage the future replacement of the existing Somatoform disorders categories with this new, poorly validated single SSD diagnostic construct, bringing ICD-10-CM in line with DSM-5.
There are implications for ICD-11, too.
Once SSD is inserted into ICD-10-CM, the presence of this term within the U.S. adaptation of ICD-10 may make it easier for ICD-11 Revision Steering Group to justify proposals to replace the existing ICD-10 Somatoform disorders categories with a single, new ICD construct contrived to incorporate SSD-like characteristics and facilitate harmonization between ICD-11 and DSM-5 disorder terms and diagnostic criteria.
+++
This post updates on proposals at the March meeting of the ICD-10-CM/PCS Coordination and Maintenance Committee to add DSM-5’s controversial new Somatic symptom disorder as an Inclusion term to ICD-10-CM.
But first, a necessary recap of the September 2013 meeting:
ICD-10-CM/PCS Coordination and Maintenance Committee meetings provide a public forum to discuss proposed changes to the U.S.’s forthcoming ICD-10-CM and ICD-10-PCS, scheduled for implementation on October 1, 2014 to be confirmed.
The public meetings, which are co-chaired by representatives for CMS and NCHS, take place in March and September and are followed by public comment periods.
The fall meeting of the ICD-10-CM/PCS Coordination and Maintenance Committee was held on September 18–19, 2013.
On Day Two of the September meeting, American Psychiatric Association’s Darrel Regier, MD, had proposed six new DSM-5 disorders for inclusion in ICD-10-CM.
On Page 45 and 46 of the Diagnosis Agenda, under Additional Tabular List Inclusion Terms for ICD-10-CM, a number of other changes to specific Chapter 5 F codes had also been proposed. These were introduced en masse, by CDC’s Donna Picket. (Reached on Day Two, at 1:22:21 in from the start of Videocast Four.)
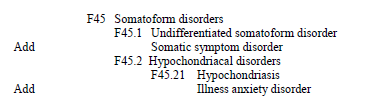
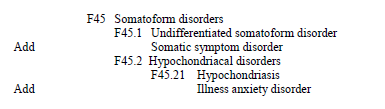
This section of the Diagnosis Agenda included the proposals to add the new DSM-5 disorders: Somatic symptom disorder (proposed to Add as an Inclusion term to F45.1 Undifferentiated somatoform disorder) and Illness anxiety disorder (proposed to Add as Inclusion term to F45.21 Hypochondriasis) to ICD-10-CM’s Chapter 5 codes.
(F45.1 and F45.21 are the ICD-10-CM codes to which these two new APA disorders are already cross-walked in the DSM-5.)
Source: Page 45,Diagnosis Agenda(Topic Packet), September 18–19, 2013 ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
+++
Videocasts of the entire September 2013 meeting proceedings, Diagnosis Agenda (Topic Packet), Procedural Agenda, Meeting materials etc can be found in Dx Revision WatchPost #277.
Note: there was no proposal at the September 2013 meeting to create a unique code for either Somatic symptom disorder (SSD) or Illness anxiety disorder, for either 2014 or October 1, 2015 implementation, and no proposal that Somatic symptom disorder should replace or subsume any of the existing ICD-10-CM F45.x Somatoform disorders. Note also, these proposals are specific to the forthcoming U.S. clinical modification of ICD-10.
In relation to the section of the Agenda on Pages 45 and 46, CDC’s, Donna Picket, had stated:
1:22:21 in: Diagnosis Agenda: “Additional Tabular List Inclusion Terms for ICD-10-CM”
Donna Pickett (CDC): “…And just to complete the package, there are other Tabular List proposals that appear on Page 45 and 46 that we would also invite your comments on. And again, with some of the terminology changes that Dr Regier has described the intent here is to make sure that if those terms are being used, that they do have a home somewhere within ICD-10-CM to facilitate people looking these up. So we invite comments. We’re showing the Tabular List proposed changes; however, there obviously would be associated Alphabetic Index changes with that which we didn’t show just to keep the package a little bit smaller…”
Source: [Unofficial transcription from Video Four, September 2013 ICD-9-CM C & M Committee meeting.]
There were no questions or comments from the floor or by phone link on any of the proposals listed on Pages 45 and 46 under “Additional Tabular List Inclusion Terms for ICD-10-CM” and no discussion or queries on any of the individual proposals listed under under this section of the Agenda between the meeting co-chairs and APA’s, Dr Regier.
NCHS’s decision on proposals to add Somatic symptom disorder (SSD) and Illness anxiety disorder as Inclusion terms to ICD-10-CM Tabular List Chapter 5, and to also add to the Index, isn’t known and may not be evident until the next ICD-10-CM Addenda is released, later this year, or until the Final Addenda released.
Some of the objections that were submitted last year to the proposal to add Somatic symptom disorder (SSD) as an Inclusion term in ICD-10-CM at the September 2013 meeting are collated on Dx Revision Watchhere.
+++
March 2014 meeting of the ICD-10-CM/PCS Coordination and Maintenance Committee
This meeting took place on March 19–20, 2014. I was unable to attend as I live in the UK.
The ICD-9-CM and ICD-10-CM Timeline and Diagnosis and Procedure Codes Agenda (Topic Packet) can be found here, on the CDC website:
A Summary Report of the Diagnosis part of the meeting is scheduled to be posted on the NCHS website, in June.
A Summary Report of the Procedure part of the meeting is scheduled to be posted on the CMS website, in June.
April 17, 2014: Deadline for receipt of public comments on proposed procedure code revisions discussed at the March 19, 2014 ICD-10 Coordination and Maintenance Committee meeting for implementation on October 1, 2014.
June 20, 2014: Deadline for receipt of public comments on proposed code revisions discussed at the March 19–20 meeting for implementation on October 1, 2015.
ICD-10-CM is currently subject to a partial code freeze. During the freeze, the public will be asked to comment on whether or not a proposal should be approved, and if not, why; and whether requests for new diagnosis or procedure codes should be created based on the criteria of the need to capture a new technology or disease. Any code requests that do not meet the criteria will be evaluated for implementation within ICD-10-CM on and after October 1, 2015 to be confirmed once the partial freeze has lifted.
Comments on the diagnosis proposals presented at the ICD Coordination and Maintenance Committee meeting should be sent, preferably by email, to the following address by June 20th deadline:nchsicd9CM@cdc.gov
+++
The Two Day proceedings were streamed live and can be watched on YouTube:
The American Psychiatric Association (APA) proposes the following addenda changes to the ICD-10-CM Tabular and Index, specifically to Chapter 5, Mental, Behavioral and Neurodevelopmental disorders (F01-F99).
The APA indicates that these revisions are necessary because DSM-5 contains several new diagnoses, as well as new disorder titles, that do not map well to any existing ICD-10-CM codes.
Because of this, they are proposing numerous new index entries and tabular inclusion terms to ensure that coders can correctly identify the codes to use. The APA proposes that these changes will also ensure that new DSM-5 disorder titles correspond to a valid ICD-10-CM code.
Many of the changes in the proposed addenda relate to the reconceptualization of the substance use disorders from having separate disorder names and codes for substance abuse and dependence. However, extensive scientific evidence was assembled to show that, rather than existing as two separate disorders, these conditions exist on a spectrum that the APA has now conceptualized as ranging from mild to moderate to severe. In order to make the closest approximations with existing ICD-10-CM codes, it is noted that codes for mild substance use disorders correspond to the abuse codes and codes for moderate and severe substance use disorders correspond to dependence codes. The APA may recommend changes in the structure and names of ICD-10-CM substance related disorders, in the future, however at the present time they are only recommending the addition of the new terminology as inclusion terms.
The following addenda are proposed for implementation on October 1, 2015
[…]
1:12:12 in from start of YouTube Three: Chapter 5 Addenda Proposed Tabular Modifications.
1:12:12 Beth Fisher (CMS): Introduces proposals for [Tabular] modifications from APA for Chapter 5. These are all Addenda type changes because [ICD-10-CM is] in code freeze mode, we didn’t have the opportunity to do new codes just yet. Hands podium to Darrel Regier, MD.
1:13:01 Darrel Regier (APA): Mapping DSM-5 to ICD-10-CM codes; Major change to rename Dementias group to Major Neurocognitive Disorders, because including in this group some neurocognitive deficit conditions such as Traumatic brain injury and other neurocognitive disorders that are not inherently some of the neurodegenerative diseases, such as Alzheimer’s, Picks Disease. (Page 64 Diagnosis Agenda)
1:14:02 Darrel Regier (APA): We’ve also introduced [in DSM-5] a Mild neurocognitive disorder that reflects the Mild cognitive impairment, MCI, that is currently in ICD-9, ICD-10…
1:15:06 Darrel Regier (APA): A lot of significant changes to substance abuse disorder area which will require some notes and guidelines…
1:15:27 Darrel Regier (APA): [APA has] a number of new disorders…15 new disorders that are in the DSM-5, but there were 50 disorders that were actually subsumed into a spectrum of conditions that dropped the total number of disorders by something like 28; so you had 50 disorders that collapsed into 22 disorders. Among those, some of the most prominent – Aspergers, Autism, Pervasive developmental disorder NOS, into a single Autism spectrum disorder…assessed on two domains…assessed in terms of level of severity instead of categorical distinctions…
1:17:04 Darrel Regier (APA): Eliminating distinction between abuse and dependence so that on a continuum of Mild, Moderate, Severe…no strict separation between abuse category and dependence…
1:21:00: Question from floor re Alcohol abuse, Alcohol dependence.
1:31:15 Beth Fisher (CDC): Some of these Inclusion terms may have been proposed at September 2013 meeting. (But does not explain the reason for their being resubmitted at the March meeting.)
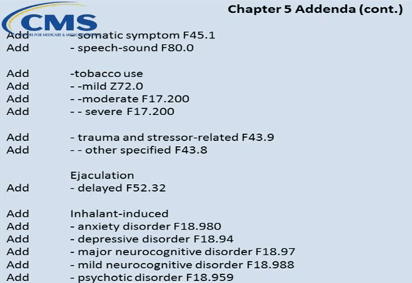
1:31:34 Beth Fisher (CDC): Begins running through all Addenda Additions.
1:31:42 Beth Fisher (CDC): At F44 Dissociative and conversion disorders, Add Conversion disorder, in parenthesis, functional neurological symptom disorder as Inclusion term.
Source: ICD-10-CM C & M Committee meeting, March 20, 2014, Screenshot Video Three
Note, there was no proposal under these Proposed Tabular Modifications to Add Somatic symptom disorder as Inclusion term to F45.1 Undifferentiated somatoform disorder to the Tabular List. But the proposal to Add Somatic symptom disorder as an Inclusion term to F45.1 Undifferentiated somatoform disorder to the Tabular List and to the Alphabetical Index had been proposed at the September 2013 meeting.
Also, no proposal to Add Illness anxiety disorder to the Tabular List, but again, this had been proposed at the September 2013 meeting (under F45.21), for both the Tabular List and the Index. (Decisions on all four of these September 2013 meeting proposals are unknown.)
Source: ICD-10-CM C & M Committee meeting, March 20, 2014, Screenshot Video Three
(No comments from floor regarding proposal to Add SSD to Index, or queries in respect of outcome of September meeting proposals. It was not feasible for me to participate in this meeting via phone link from UK to query.)
Note, there was no proposal under Proposed Index Modifications to add Illness anxiety disorder to the Index, but this proposal had been included in the September 2013 Topic Packet. Why SSD has been resubmitted for consideration for addition to the Index at the March 2014 meeting is unclear, and as I say, the outcome of proposals for the September meeting for both SSD and IAD to be added to both Tabular List and to Index is unknown.
1:44:26: Questions from floor regarding Alcohol; Cannabis; Cocaine use; Implications for legal differences between states for use of cannabis. Question regarding Neurodegeneration due to alcohol.
1:50.02 Beth Fisher (CMS): Other Addenda (Ed: presumably Tab and Index Addenda on pp 91–93 and 93–97) were reached on Day One, as there was time, so not being presenting on Day Two. Invites further comments.
1:50.27 Donna Picket (CDC): Adjourns meeting. Reminds floor (and participants via phone link/videocasts and non attendees), to submit comments on Diagnosis proposals by June 20 deadline.
1:51:07 Question from floor: Process question: if these proposals are all approved, when will they be approved and when will they be effective, because we want to notify our members of what codes to use?
1:51:32: Donna Pickett (CDC): All of these being presented were for consideration for implementation in October 1, 2015. Within 2015, we have a huge body of work that has been accumulating during partial code freeze and we’ve encouraged comments to come in about the timing for making the Final Addenda available. The typical time frame we have used in the past is posting [Addenda] in June and proposals to become effective October 1, of that same year. However, issues have arisen because there is a huge body of work and it was mentioned, yesterday, [during Meeting Day One] that the industry may want to have an Addenda released earlier and we invited comment on that, because of the amount of work that would need to go into incorporating the changes into the relevant systems and programs etc. If we were to stay with the traditional process, the Addenda would be made available in June. Meeting concluded.
Comments on the diagnosis proposals presented at the ICD-10-CM Coordination and Maintenance Committee meeting should be sent, preferably by email, to the following address by June 20th deadline:nchsicd9CM@cdc.gov
This list of tentative diagnosis agenda topics is not final. The final topics material will be available electronically from the NCHS web site prior to the meeting.
If you are unable to attend the meeting in person there will be conference lines available on the day of the meeting. Individuals do not need to register on line for the meeting if planning to dial in.
The next meeting of the ICD-10-CM/PCS Coordination and Maintenance Committee is scheduled for March 19–20, 2014. If you are planning to attend the meeting in person you will need to register, online, by March 14.
Public forum to discuss proposed changes to ICD-10-CM and ICD-10-PCS
Wednesday, March 19, 2014 – Thursday, March 2o, 2014
CMS Auditorium, Baltimore, MD
Agendas for the meeting will be posted in February 2014.
If phone lines and live webinar are made available the information will be posted closer to the meeting date.
Day One | Time: 03/19/2014 9:00 AM – 5:00 PM CMS Auditorium
Session: ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
The first day of the meeting, March 19, 2014, will be devoted to procedure code issues.
Day Two | Time: 03/20/2014 9:00 AM – 5:00 PM CMS Auditorium
Session: ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
The second day of the meeting, March 20, 2014 will be devoted to diagnosis code topics.
+++
The National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS) are the U.S. governmental agencies responsible for overseeing all changes and modifications to the ICD-9-CM and draft ICD-10-CM/PCS.
NCHS is also responsible for the development of ICD-10-CM, adapted from the WHO’s ICD-10 for U.S. specific use.
The 2014 release of the draft ICD-10-CM (which replaces the July 2013 release) can be viewed or downloaded here.
ICD-10-CM is scheduled for implementation on October 1, 2014. Until that time the codes in ICD-10-CM are not valid for any purpose or use.
New concepts are added to ICD-10-CM based on the established update process for ICD-9-CM (the ICD-9-CM Coordination and Maintenance Committee) and the World Health Organization’s ICD-10 (the Update and Revision Committee).
Meetings of the Coordination and Maintenance Committee are co-chaired by a representative from NCHS and from CMS. Responsibility for maintenance of the ICD-9-CM is divided between these two agencies, with classification of diagnoses by NCHS and procedures by CMS.
The name of the Committee will change to the ICD-10-CM/PCS Coordination and Maintenance Committee with the March meeting, as the last updates to ICD-9-CM/PCS took place on October 1, 2013.
Meetings are held twice yearly, in public, at CMS headquarters in Baltimore, MD. The next meeting is scheduled for March 19–20, 2014. The fall meeting is scheduled for September 23–24, 2014.
The Committee provides a public forum to discuss proposed modifications, code changes, updates and corrections to the diagnosis codes in ICD-10-CM and procedural codes in ICD-10-PCS.
Public participation can also take place via phone conference link and live webinar. (Details for both in the Agenda documents.)
Agendas are posted approximately one month prior to the meetings. Diagnostic and procedural proposal Topic Packets, meeting materials, hand outs and presentation slides are posted on the CDC and CMS websites shortly before a meeting.
Up until 2011, transcripts of meeting proceedings were provided. Provision of transcripts is now replaced with videocasts for the full, two-day proceedings, available from the CMS website and posted on YouTube, and a brief Meeting Summary report, available from the CDC site shortly after the meeting.
For attendance in person, prior registration is required, via the CMS meeting registration website. Registration opens approximately one month prior to a meeting and closes a few days before Day One of a meeting.
+++
Proposals for modifications, additions, corrections
Suggestions for modifications to ICD-10-CM/PCS come from both the public and private sectors. Since the draft ICD-10-CM is adapted from the WHO’s ICD-10, which is subject to an annual update process, some proposed modifications to ICD-10-CM may reflect updates to the ICD-10.
Interested parties (requestors) must submit proposals for modifications prior to a scheduled meeting and by a specific date. Proposals should be consistent with the structure and conventions of the classification. See Submission of Proposals for submission requirements and proposal samples.
Once proposals have been reviewed, requestors are contacted as to whether their proposal has been approved for presentation at the next Coordination and Maintenance Committee meeting or not.
Approved proposals are presented at the meetings by representatives for professional bodies, advocacy organizations, clinicians, other professional stakeholders or members of the public with an interest, or are sometimes presented by an NCHS/CMS representative on behalf of a requestor.
No decisions on proposed modifications are made at the meetings. Recommendations and comments are reviewed and evaluated, once the comment period has closed, before final decisions are made.
The Coordination and Maintenance Committee’s role is advisory. All final decisions are made by the Director of NCHS and Administrator of CMS.
Final decisions are made at the end of the year and become effective October 1 of the following year.
+++
Submitting written comment on proposals presented at meetings
Comments on proposals are invited, at the meeting, at the end of each presentation, or may be submitted in writing following the meeting, during a one to two month duration public comment period.
Addresses for submitting comments are included in the Agenda Topic Packets published before the meetings. NCHS/CMS state that electronic submissions are greatly preferred over snail mail in order to ensure timely receipt of responses.
+++
Partial code freeze and timing of proposals
According to the Summary of Diagnosis Presentations for the September 18–19, 2013 meeting (for which the comment period closed on November 15):
“Except where noted, all topics are being considered for implementation on October 1, 2015. The addenda items are being considered for implementation prior to October 1, 2014.”
(“ICD-10-CM TABULAR OF DISEASES – PROPOSED ADDENDA” Tabular and Index modification proposals are set out on Diagnosis Agenda Pages 60-66.)
Note that some proposals in the Diagnosis Agenda were requested for insertion in October 2014 as Inclusion Terms to existing codes, with new codes proposed to be created for October 2015, notably, the 6 proposals to insert new DSM-5 disorders into ICD-10-CM presented by Darrel Regier, MD, on behalf of the American Psychiatric Association (Diagnosis Agenda Pages 32-44).
For the September 18–19, 2013 meeting, when submitting written comments, responders were asked to consider the following:
Whether they agree with a proposal, disagree (and why), or have an alternative proposal to suggest. But were also invited to comment on the timing of those proposals that were being requested for approval for October 2014:
Does a request for a new diagnosis or procedure code meet the criteria for implementation in October 2014 during apartial code freeze*based on the criteria of the need to capture a new technology or disease; or should consideration for approval be deferred to October 2015? And separately, to comment on the creation of a specific new code for the condition effective from October 1, 2015 (where requested).
Any code requests that do not meet the criteria [for inclusion during a partial freeze] will be evaluated for implementation within ICD-10-CM on and after October 1, 2015 once the partial freeze has ended and regular (at least annual) updates to ICD-10-CM/PCS resume.
October 1, 2011 is the last major update of ICD-9-CM. Any further revisions to ICD-9-CM will only be for a new disease and/or a procedure representing new technology. Revisions will be posted on this website as addenda (revisions to procedures are posted on the CMS website).
After October 1, 2011 there will be no further release of ICD-9-CM on CD-ROM.
October 1, 2011 is the last major update of ICD-10-CM/PCS until October 1, 2015.
Between October 1, 2011 and October 1, 2015 revisions to ICD-10-CM/PCS will be for new diseases/new technology procedures, and any minor revisions to correct reported errors in these classifications.
Regular (at least annual) updates to ICD-10-CM/PCS will resume on October 1, 2015.
+++ Public comments not made public
Note that written public comments received by NCHS (Diagnosis) and CMS (Procedural) on proposals requested via these meetings are not aggregated and made publicly accessible. Nor are the names of organizations, professional bodies, individuals or others who have submitted comments listed publicly. It is not possible to scrutinize the number, provenance or substance of the comments received in support of, or in opposition to requests for modifications to ICD-10-CM presented via these meetings. Nor are NCHS/CMS’s rationales for the approval or rejection of requests for modifications to diagnosis or procedural codes on public record.
+++
September 18–19, 2013 meeting
A substantial number of modifications were proposed via the September 2013 meeting for both procedural and diagnosis codes. These are set out in the Agenda/Topic Packet PDF documents:
Go here for registration details. (CMS confirmed to me via email on 01.23.13 that the deadline for registration is March 14, not February 14, as incorrectly published in the Diagnosis Agenda timeline.)
April 18, 2014: deadline for receipt of public comments on proposed codes and modifications tabled for March meeting. (Note there is only a 4 week period following this meeting during which written comments can be submitted.)
+++
Key ICD-10-CM/PCS Timeline dates extracted from full timeline, Pages 3-8, September 18-19, 2013 Diagnosis Agenda
March 19–20, 2014: ICD-10-CM/PCS Coordination and Maintenance Committee meeting.
April 1, 2014: There will be no new ICD-9-CM codes to capture new diseases or technology on April 1, 2014, since the last updates to ICD-9-CM will take place on October 1, 2013.
April 2014: Notice of Proposed Rulemaking to be published in the Federal Register as mandated by Public Law 99-509. This notice will include references to the complete and finalized FY 2015 ICD-10-CM diagnosis and ICD-10-PCS procedure codes. It will also include proposed revisions to the MS-DRG system based on ICD-10-CM/PCS codes on which the public may comment. The proposed rule can be accessed at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html?redirect=/AcuteInpatientPPS/IPPS/list.asp
April 18, 2014: Deadline for receipt of public comments on proposed code [at March meeting.]
June 2014: Final addendum posted on web pages as follows:
November 2014: Any new ICD-10 codes required to capture new technology that will be implemented on the following April 1 will be announced. Information on any new codes to be implemented April 1, 2015 will be posted on the following websites:
Since my update on January 3, in the ICD-11 Beta draft, Hypochondriasis (illness anxiety disorder) has since been reverted to Hypochondriasis with illness anxiety disorder listed, instead, as an Inclusion term to Hypochondriasis.
Hypochondriasis was subsequently assigned to three parents:
Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere; Obsessive-compulsive and related disorders; Anxiety and fear-related disorders;
At February 3, Hypochondriasis has been removed from parent Bodily distress disorders and is currently assigned dual parentage under:
Obsessive-compulsive and related disorders; Anxiety and fear-related disorders
The Definition for Hypochondriasis currently displaying in the Beta draft appears to be the legacy Definition, unrevised from ICD-10.
Update to ICD-11 Beta draft at January 3, 2014:
Revision to ICD-11 Beta draft: In the report below, I stated:
ICD-11 public version Beta draft:Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
As the ICD-11 Beta drafting platform now stands, at January 3, 2014, the DSM-5 term “(illness anxiety disorder)” has been removed from the “Hypochondriasis(illness anxiety disorder)” disorder name and the term reverted to Hypochondriasis.
The term “illness anxiety disorder” is now displaying as listed under “Synonyms” to Hypochondriasis in the ICD-11 Beta Foundation View, and listed under “All Index Terms” in the Morbidity Linearization View.
I also set out how public and professional stakeholders can submit comment or objections on any of the proposals requested at this meeting before the November 15 deadline.
At the September meeting, Darrel Regier, MD, APA Director of Research, presented six diagnoses that are new to DSM-5 for inclusion within ICD-10-CM, with proposals for assigning unique new codes to these disorders for October 2015 [1].
Some of the DSM-5 disorders, below, presented for consideration for inclusion in ICD-10-CM are already entered into the ICD-11 Beta drafting platform and in some cases, entered into the draft over a year or more ago.*
*Caveat: The ICD-11 Beta draft is not approved by WHO or WHA. The Beta draft is a work in progress over the next two to three years. The Beta draft is updated on a daily basis: parent terms, category terms, sorting codes and descriptive content are subject to change as chapter reorganization progresses. This post reflects the Beta draft as it stood on November 6, 2013. ICD-11 Beta Draft Caveats
Proposal for ICD-10-CM for October 1, 2014: add Binge eating disorder (BED) as an inclusion term to F50.8 Other eating disorders.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created for F50.81 Binge eating disorder.
ICD-11 public version Beta draft: Binge eating disorder currently proposed to be coded under Feeding and eating disorders and assigned a unique ICD-11 code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Binge eating disorder.
——————————
Gender Identity Disorder in Adolescence and Adulthood
Proposal for ICD-10-CM for October 1, 2014: that ICD-10-CM change the code for Gender identity disorder in adolescents and adulthood to F64.0 and that “gender dysphoria in adolescents and adults” is added as an inclusion term for this entry.
Source: September 2013 Diagnosis Agenda, Page 34
[See Page 34 of Diagnosis Agenda for discussion of proposed coding changes.]
Proposal for ICD-10-CM for October 1, 2014: add Disruptive mood dysregulation disorder (DMDD) as an inclusion term under F34.8: Other persistent mood [affective] disorders.
Proposal for ICD-10-CM for October 1, 2015: that unique new codes are created at F34.81 Disruptive mood dysregulation disorder and F34.89 Other specified persistent mood disorders.
ICD-11 public version Beta draft:Disruptive mood dysregulation disorder (DMDD) is not currently listed.
Proposal for ICD-10-CM for October 1, 2014: add Social (Pragmatic) Communication Disorder as an inclusion term under F80.89 Other developmental disorders of speech and language.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F80.82 Social pragmatic communication disorder.
Excludes1: Asperger’s syndrome (F84.5)
Autistic disorder (F84.0)
ICD-11 public version Beta draft: Social (Pragmatic) Communication Disorder is not currently listed.
Proposal for ICD-10-CM for October 1, 2014: add Hoarding disorder as an inclusion term to F42 Obsessive Compulsive Disorder.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.2 for Obsessive Compulsive Disorder and F42.3 for Hoarding Disorder in future revisions. (Ms. Pickett stated that new code proposal starting at F42.2 is due to F42.0 and F42.1 deactivation by WHO.)
F42 Obsessive compulsive disorder
New code F42.2 Mixed obsessional thoughts and acts
New code F42.3 Hoarding disorder
New code F42.8 Other obsessive compulsive disorder
New code F42.9 Obsessive-compulsive disorder, unspecified
ICD-11 public version Beta draft: Hoarding disorder currently proposed to be coded under parent Obsessive-compulsive and related disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Hoarding disorder.
Proposal for ICD-10-CM for October 1, 2014: add Excoriation (skin-picking) disorder as an inclusion term to L98.1 Factitial dermatitis (Dermatology section).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.4 Excoriation (skin-picking) disorder.
Excludes1: Factitial dermatitis (L98.1)
Other specified behavioral and emotional disorders with onset usually occurring in early childhood and adolescence (F98.8)
ICD-11 public version Beta draft: Excoriation disorder (skin-picking disorder) currently proposed to be coded under Obsessive-compulsive and related disorders under parent Body-focused repetitive behaviour disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Excoriation (skin-picking) disorder.
APA considers that placing PMDD outside the recurrent depressive disorder category is less than optimal for differentiating it from ICD-10-CM N94.3 Premenstrual Tension Syndrome, which is generally less severe than PMDD, and does not require psychiatric treatment. If an alternative code in the F32 series is possible, APA would prefer to modify the code in that section in future revisions.
Proposal for ICD-10-CM for October 1, 2014: add Premenstrual dysphoric disorder as an inclusion term to N94.3 Premenstrual tension syndrome (Chapter 15 Diseases of the genitourinary system).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created under Chapter 5 F32.8 Other depressive episodes.
New code F32.81 Premenstrual dysphoric disorder
Excludes1: premenstrual tension syndrome (N94.3)
ICD-11 public version Beta draft:Premenstrual dysphoric disorder (PMDD) currently proposed to be dual coded under Chapter 15 Diseases of the genitourinary system > Premenstrual tension syndrome and also coded under Chapter 5 Depressive disorders and assigned a unique code. A draft ICD-11 Definition has been populated for PMDD but no other ICD-11 “Content Model” descriptive parameters have been populated.
——————————
Somatic symptom disorder and Illness anxiety disorder
Source: September 2013 Diagnosis Agenda, Page 45
Somatic symptom disorder:
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Somatic symptom disorder under F45 Somatoform Disorders as inclusion term to F45.1 Undifferentiated somatoform disorder.
ICD-11 public version Beta draft: There is no Somatic symptom disorder in the ICD-11 Beta draft either as a unique new ICD-11 entity code or as an inclusion term or Synonym to an existing ICD-11 code.
For ICD-11 Core version: the current proposal for the F45 Somatoform disorders is for a proposed new construct, Bodily distress disorder, to replace a number of existing ICD-10 categories under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere. Two specifiers: Bodily distress disorder and Severe Bodily distress disorder have yet to be defined or characterized within the Beta draft and no “Content Model” parameters have yet been populated. ICD-11 plans to field test this proposed new ICD-11 construct.
The Definition for Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere currently displaying in the Beta draft appears to be the legacy Somatoform disorders Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
——————————
Illness anxiety disorder
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Illness anxiety disorder under F45 Somatoform disorders as inclusion term to F45.21 Hypochondriasis.
ICD-11 public version Beta draft:Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
The Definition for Hypochondriasis (illness anxiety disorder) currently displaying in the Beta draft appears to be the legacy Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
Submitting comments
If you have comments or objections to any of the proposals requested at the September ICD-9-CM C & M Committee meeting, the deadline for submissions is November 15, by email, to Donna Pickett: nchsicd9CM@cdc.gov


Which new DSM-5 disorders proposed for inserting into ICD-10-CM are already added to the ICD-11 Beta draft?
November 6, 2013 by admindxrw
Post #280 Shortlink: http://wp.me/pKrrB-3vs
Update to ICD-11 Beta draft at February 3, 2014:
Since my update on January 3, in the ICD-11 Beta draft, Hypochondriasis (illness anxiety disorder) has since been reverted to Hypochondriasis with illness anxiety disorder listed, instead, as an Inclusion term to Hypochondriasis.
Hypochondriasis was subsequently assigned to three parents:
Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere; Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders;
At February 3, Hypochondriasis has been removed from parent Bodily distress disorders and is currently assigned dual parentage under:
Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders
Foundation View:
hppt://apps.who.int/classifications/icd11/browse/f/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
Joint Linearization for Mortality and Morbidity Statistics View:
http://apps.who.int/classifications/icd11/browse/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
The Definition for Hypochondriasis currently displaying in the Beta draft appears to be the legacy Definition, unrevised from ICD-10.
Update to ICD-11 Beta draft at January 3, 2014:
Revision to ICD-11 Beta draft: In the report below, I stated:
As the ICD-11 Beta drafting platform now stands, at January 3, 2014, the DSM-5 term “(illness anxiety disorder)” has been removed from the “Hypochondriasis (illness anxiety disorder)” disorder name and the term reverted to Hypochondriasis.
The term “illness anxiety disorder” is now displaying as listed under “Synonyms” to Hypochondriasis in the ICD-11 Beta Foundation View, and listed under “All Index Terms” in the Morbidity Linearization View.
As previously posted on November 6, 2013:
In the previous four posts, I have documented the September 18-19, 2013 meeting of the ICD-9-CM Coordination and Maintenance Committee and reported on American Psychiatric Association (APA) proposals for inserting a number of new DSM-5 terms into the forthcoming US specific ICD-10-CM.
I also set out how public and professional stakeholders can submit comment or objections on any of the proposals requested at this meeting before the November 15 deadline.
At the September meeting, Darrel Regier, MD, APA Director of Research, presented six diagnoses that are new to DSM-5 for inclusion within ICD-10-CM, with proposals for assigning unique new codes to these disorders for October 2015 [1].
Some of the DSM-5 disorders, below, presented for consideration for inclusion in ICD-10-CM are already entered into the ICD-11 Beta drafting platform and in some cases, entered into the draft over a year or more ago.*
Binge eating disorder (BED)
(Rationale: Page 32, Diagnosis Agenda: Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Binge eating disorder (BED) as an inclusion term to F50.8 Other eating disorders.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created for F50.81 Binge eating disorder.
ICD-11 public version Beta draft: Binge eating disorder currently proposed to be coded under Feeding and eating disorders and assigned a unique ICD-11 code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Binge eating disorder.
——————————
Gender Identity Disorder in Adolescence and Adulthood
(Rationale: Page 34, Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: that ICD-10-CM change the code for Gender identity disorder in adolescents and adulthood to F64.0 and that “gender dysphoria in adolescents and adults” is added as an inclusion term for this entry.
Source: September 2013 Diagnosis Agenda, Page 34
[See Page 34 of Diagnosis Agenda for discussion of proposed coding changes.]
——————————
Disruptive mood dysregulation disorder (DMDD)
(Rationale: Page 35, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Disruptive mood dysregulation disorder (DMDD) as an inclusion term under F34.8: Other persistent mood [affective] disorders.
Proposal for ICD-10-CM for October 1, 2015: that unique new codes are created at F34.81 Disruptive mood dysregulation disorder and F34.89 Other specified persistent mood disorders.
ICD-11 public version Beta draft: Disruptive mood dysregulation disorder (DMDD) is not currently listed.
——————————
Social (Pragmatic) Communication Disorder
(Rationale: Page 37, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Social (Pragmatic) Communication Disorder as an inclusion term under F80.89 Other developmental disorders of speech and language.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F80.82 Social pragmatic communication disorder.
Excludes1: Asperger’s syndrome (F84.5)
Autistic disorder (F84.0)
ICD-11 public version Beta draft: Social (Pragmatic) Communication Disorder is not currently listed.
——————————
Hoarding disorder
(Rationale: Page 39, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Hoarding disorder as an inclusion term to F42 Obsessive Compulsive Disorder.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.2 for Obsessive Compulsive Disorder and F42.3 for Hoarding Disorder in future revisions. (Ms. Pickett stated that new code proposal starting at F42.2 is due to F42.0 and F42.1 deactivation by WHO.)
F42 Obsessive compulsive disorder
New code F42.2 Mixed obsessional thoughts and acts
New code F42.3 Hoarding disorder
New code F42.8 Other obsessive compulsive disorder
New code F42.9 Obsessive-compulsive disorder, unspecified
ICD-11 public version Beta draft: Hoarding disorder currently proposed to be coded under parent Obsessive-compulsive and related disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Hoarding disorder.
——————————
Excoriation (skin picking) disorder
(APA Rationale: Page 41, Diagnosis Agenda, Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Excoriation (skin-picking) disorder as an inclusion term to L98.1 Factitial dermatitis (Dermatology section).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.4 Excoriation (skin-picking) disorder.
Excludes1: Factitial dermatitis (L98.1)
Other specified behavioral and emotional disorders with onset usually occurring in early childhood and adolescence (F98.8)
ICD-11 public version Beta draft: Excoriation disorder (skin-picking disorder) currently proposed to be coded under Obsessive-compulsive and related disorders under parent Body-focused repetitive behaviour disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Excoriation (skin-picking) disorder.
——————————
Premenstrual dysphoric disorder (PMDD)
(APA Rationale: Page 43, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
APA considers that placing PMDD outside the recurrent depressive disorder category is less than optimal for differentiating it from ICD-10-CM N94.3 Premenstrual Tension Syndrome, which is generally less severe than PMDD, and does not require psychiatric treatment. If an alternative code in the F32 series is possible, APA would prefer to modify the code in that section in future revisions.
Proposal for ICD-10-CM for October 1, 2014: add Premenstrual dysphoric disorder as an inclusion term to N94.3 Premenstrual tension syndrome (Chapter 15 Diseases of the genitourinary system).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created under Chapter 5 F32.8 Other depressive episodes.
New code F32.81 Premenstrual dysphoric disorder
Excludes1: premenstrual tension syndrome (N94.3)
ICD-11 public version Beta draft: Premenstrual dysphoric disorder (PMDD) currently proposed to be dual coded under Chapter 15 Diseases of the genitourinary system > Premenstrual tension syndrome and also coded under Chapter 5 Depressive disorders and assigned a unique code. A draft ICD-11 Definition has been populated for PMDD but no other ICD-11 “Content Model” descriptive parameters have been populated.
——————————
Somatic symptom disorder and Illness anxiety disorder
Source: September 2013 Diagnosis Agenda, Page 45
Somatic symptom disorder:
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Somatic symptom disorder under F45 Somatoform Disorders as inclusion term to F45.1 Undifferentiated somatoform disorder.
ICD-11 public version Beta draft: There is no Somatic symptom disorder in the ICD-11 Beta draft either as a unique new ICD-11 entity code or as an inclusion term or Synonym to an existing ICD-11 code.
For ICD-11 Core version: the current proposal for the F45 Somatoform disorders is for a proposed new construct, Bodily distress disorder, to replace a number of existing ICD-10 categories under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere. Two specifiers: Bodily distress disorder and Severe Bodily distress disorder have yet to be defined or characterized within the Beta draft and no “Content Model” parameters have yet been populated. ICD-11 plans to field test this proposed new ICD-11 construct.
The Definition for Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere currently displaying in the Beta draft appears to be the legacy Somatoform disorders Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
——————————
Illness anxiety disorder
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Illness anxiety disorder under F45 Somatoform disorders as inclusion term to F45.21 Hypochondriasis.
ICD-11 public version Beta draft: Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
The Definition for Hypochondriasis (illness anxiety disorder) currently displaying in the Beta draft appears to be the legacy Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
Submitting comments
If you have comments or objections to any of the proposals requested at the September ICD-9-CM C & M Committee meeting, the deadline for submissions is November 15, by email, to Donna Pickett: nchsicd9CM@cdc.gov
+++
References for key documents:
1. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1750103
2. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm#public_meetings
September meeting Proposals [PDF – 342 KB]
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
September meeting Summary of Diagnosis Presentations PDF file [PDF – 347 KB]:
http://www.cdc.gov/nchs/data/icd/icd_summary_sept_181913.pdf
3. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18-19, 2013 meeting materials and four YouTubes of proceedings:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/ICD-9-CM-C-and-M-Meeting-Materials-Items/2013-09-18-MeetingMaterials.html
4. September 19, 2013 Meeting Day Two: ICD-9-CM Coordination and Maintenance Committee Meeting Part 4 videocast:
http://www.youtube.com/watch?v=G-pYdKyr_NE
5. ICD-11 Beta drafting platform (public version):
http://apps.who.int/classifications/icd11/browse/f/en
Share this:
Filed under American Psychiatric Association (APA), CDC, CMS, Criticism of DSM-V, DSM-5, DSM-5, ICD-10-CM, ICD-10-PCS, ICD-11, Somatic Symptom Disorder, WHO (World Health Organization) Tagged with american psychiatric association, binge eating disorder, disruptive mood dysregulation disorder, dsm-5, icd-10-cm, institute of psychiatry, NCHS, premenstrual dysphoric disorder, public comment, somatic symptom disorder