Videos and meeting materials: September 18–19 ICD-9-CM Coordination and Maintenance Committee meeting
October 10, 2013
Post #277 Shortlink: http://wp.me/pKrrB-3tV
Update: Crazy Like Us: How the U.S. Exports Its Models of Illness – DSM-5 is Americanizing the world’s understanding of the mind by Christopher Lane, Ph.D. in Side Effects, October 9, 2013
This report relates to proposals submitted via the September ICD-9-CM/PCS Coordination and Maintenance Committee meeting for the inclusion of additional codes to the forthcoming US specific ICD-10-CM.
The twice yearly ICD-9-CM Coordination and Maintenance Committee meetings provide a public forum to discuss proposed code changes to ICD-9-CM and the ICD-10-CM/PCS. Next year, the committee, which is co-chaired by CMS and CDC, will be renamed to the ICD-10-CM Coordination and Maintenance Committee.
ICD-10-CM/PCS is scheduled for implementation in October 2014 and currently subject to partial code freeze.
The meeting scheduled on September 18, 2013 was devoted to both diagnosis and procedure code topics. The second day of the meeting, September 19, continued discussions related to diagnosis code topics.
Below are links for key meeting materials, four videocasts, and agenda item listings for the diagnosis proposals presented on Day Two (videocast Part 4). This includes the presentation of proposals by American Psychiatric Association (APA) Director of Research, Darrel Regier, MD, for insertion of new DSM-5 diagnoses into the ICD-10-CM.
Meeting materials:
From CDC website: ICD-9-CM Coordination and Maintenance Committee webpage:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm
September 18-19, 2013 meeting Proposals (Timeline, Agenda for Diagnosis Proposals) [PDF – 342 KB]
From CMS.gov website:
September 18-19, 2013 meeting materials page
September 18, 2013 Agenda (Timeline, Agenda for ICD-10-PCS Topics, Procedure presentations) [PDF, 326KB]
September 18, 2013 Meeting Materials [ZIP, 4MB]
Download Zip file from CMS.gov meeting materials page | 4MB Zip file unpacks to:
PDF Presenter Slides: Cerapedics ICD-9 9 18 2013 FINAL [712KB]
PDF Presenter Slides: Respicardia ICD-9 Sept 18 FINAL [670KB]
PDF CMS/CDC Meeting Slides: September-ICD9CM-slides [3033KB]
PDF Text version of CMS/CDC Meeting slides: 508-Compliant-Version-of-September-ICD9CM-slides [282KB]
Videocasts for September 18, 2013 | Day One
Pat Brooks (CMS) Co-Chairperson
9:00 AM – 12:30 PM ICD-10-PCS Procedure presentations with public comment
12:30 PM – 1:30 PM Lunch break
1:30 PM – 5:00 PM Diagnosis presentations with public comment
Part 1 1:43 hours duration
Procedure presentations with public comment
Part 2 1:27 hours duration
Procedure presentations with public comment
Part 3 59 minutes duration
Diagnosis presentations with public comment
Videocast for September 19, 2013 | Day Two
Donna Pickett (CDC) Co-Chairperson
Part 4 1:42 hours duration
Diagnosis presentations with public comment
Diagnosis proposals
4:58 mins in: Presenter Lizabeth (Beth) Fisher (CDC) [on behalf of requestor: The American Society of Anesthesiologists]
Page 47 Diagnosis Agenda: Unintended awareness under general anesthesia
Comment from floor: Robert Adams reads out written statement.
13:56 mins in: DSM-5 and ICD-10-CM Discussions on mental health conditions and harmonization with ICD-10-CM.
Presenter: Darrel Regier, MD (Director of Research, APA; served as DSM-5 Task Force Vice-Chair)
Preamble about DSM and DSM-5.
Page 32 Diagnosis Agenda: Binge eating disorder
No questions or comments from the floor or by phone link.
29 mins in: Page 34 Diagnosis Agenda: Gender identity disorder in adolescence and adulthood
No questions or comments from the floor or by phone link.
37 mins in: Page 35 Diagnosis Agenda: Disruptive mood dysregulation disorder (DMDD)
No questions or comments from the floor or by phone link.
45 mins in: Page 37 Diagnosis Agenda: Social (pragmatic) communication disorder
No questions or comments from the floor or by phone link.
54 mins in: Page 39 Diagnosis Agenda: Hoarding disorder
No questions or comments from the floor or by phone link.
1hr:1 min in: Page 41 Diagnosis Agenda: Excoriation (skin picking) disorder
Some questions raised by DP on behalf of other and comment from the floor.
1hr:14 mins in: Page 43 Diagnosis Agenda: Premenstrual dysphoric disorder (PMDD)
Question raised by DP regarding PMDD and Excludes.
No questions or comments from the floor or by phone link.
Dr Regier concludes his presentation and hands podium back to Donna Pickett (CDC).
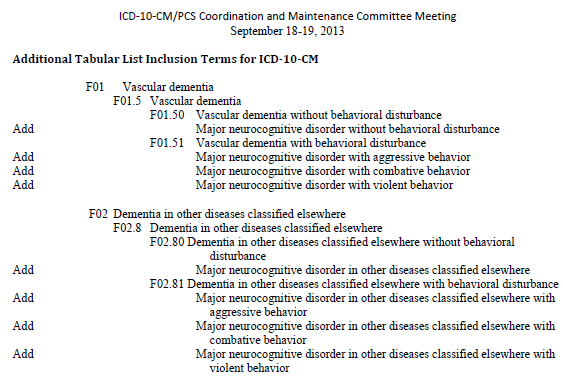
1hr:22 mins in: Page 45-46 Diagnosis Agenda: Additional Tabular List Inclusion Terms for ICD-10-CM
See screenshots at end of Post #276 for Diagnosis Agenda Pages 45-46.
[Unofficial transcription from videocast]
Donna Pickett (CDC): “…And just to complete the package, there are other Tabular List proposals that appear on Page 45 and 46 that we would also invite your comments on. And again, with some of the terminology changes that Dr Regier has described the intent here is to make sure that if those terms are being used, that they do have a home somewhere within ICD-10-CM to facilitate people looking these up. So we invite comments. We’re showing the Tabular List proposed changes; however, there obviously would be associated Alphabetic Index changes with that which we didn’t show just to keep the package a little bit smaller…”
No questions or comments from the floor or by phone link on any of the proposed inclusion terms listed on Pages 45 and 46 under “Additional Tabular List Inclusion Terms for ICD-10-CM”.
Donna Picket moves on to next set of proposals and turns podium over to Beth Fisher (CDC).
1hr:23 mins in: Page 49 Diagnosis Agenda: Intracranial injury (TBI)
Comment from floor at 1hr:32 mins: Luana Ciccarelli from the American Academy of Neurology. Comment from Sue Bowman read out by Beth Fisher.
1hr:34 mins in: Page 53 Diagnosis Agenda: Placenta Previa vs Low Lying Placenta
Presenter Lizabeth (Beth) Fisher (CDC) on behalf of requestor: The American Congress of Obstetricians and Gynecologists (ACOG).
No questions or comments from the floor or by phone link.
This concluded the diagnosis portion of the presentations.
Note that Agenda items from Page 53 onwards were tabled for presentation and discussion in earlier in the meeting proceedings.
1hr:40 mins in: Donna Pickett (CDC) brings meeting to a close.
[Unofficial transcription from videocast]
Donna Pickett (CDC): “…November 15…is in the Topic Package for receipt of comments on all of the proposals. That is the deadline, but we’d love to have them sooner as this does have implications in terms of what does become part of an addenda or not, and that would be specific to the inclusion terms in the Tabular List and Alphabetical Index because, again, unless the proposal meets the criteria established for the partial freeze, no new codes are being entertained except for the ones that were requested. We invite your comments on that as well…”
Submitting public comment:
The deadline for receipt of public and professional stakeholder comment on any of the proposed ICD-10-CM/PCS code revisions discussed at the September 18-19, 2013 ICD-9-CM Coordination and Maintenance Committee meeting is November 15.
Comments should be sent to the following dedicated NCHS/CMS email addresses:
Procedure comments by email to Pat Brooks, CMS: patricia.brooks2@cms.hss.gov
Diagnosis comments by email to Donna Pickett, CDC: nchsicd9CM@cdc.gov
(Full contact details for submission of written comments/objections to NCHS/CMS on Page 8 of the Proposals/Diagnosis Agenda PDF. Electronic submissions are much preferred in order to ensure timely receipt.)


Keep SSD out of ICD-10-CM – November 15 deadline for objections
November 1, 2013 by admindxrw
Post #278 Shortlink: http://wp.me/pKrrB-3vK
Update: My submission on behalf of Dx Revision Watch can be read here.
The American Psychiatric Association (APA) has proposed the following DSM-5 disorders for inclusion in the forthcoming ICD-10-CM (Pages 32-44, September 2013 Diagnosis Agenda):
Additionally, APA has petitioned for revisions to the ICD-10-CM listing for gender dysphoria in adolescents and adults, which is not a new disorder.
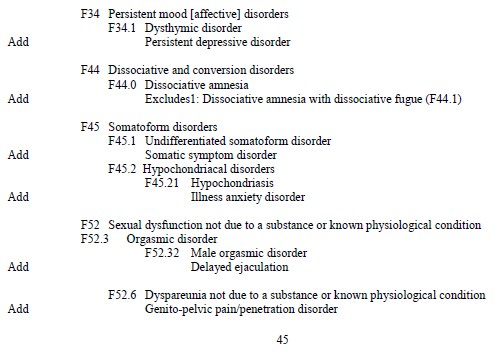
On Page 45 and 46 of the Agenda, under Additional Tabular List Inclusion Terms for ICD-10-CM a number of other additions and changes to specific Chapter 5 F codes are being proposed, including the insertion of Somatic symptom disorder (SSD) and Illness anxiety disorder.
+++
A final reminder of the deadline for comments and objections in relation to Somatic symptom disorder
Q: When do objections need to be in by and where should they be sent?
A: Submit objections via email by November 15 to Donna Pickett, CDC: nchsicd9CM@cdc.gov
Q: Can anyone submit objections?
A: Yes. And from as many patient, professional and advocacy groups as possible, particularly from the U.S. but also international objections. Although this concerns potential changes to the draft of the U.S. specific ICD-10-CM there may be implications for ICD-11.
Q: What is being proposed?
A: The American Psychiatric Association has requested 6 new DSM-5 disorders for consideration for inclusion in the forthcoming ICD-10-CM via the September 18-19, 2013 ICD-9-CM Coordination and Maintenance Committee meeting.
APA’s rationales for these requested additions, the coding proposals and timings are set out on Pages 32 thru 44 of the September meeting Diagnosis Agenda.
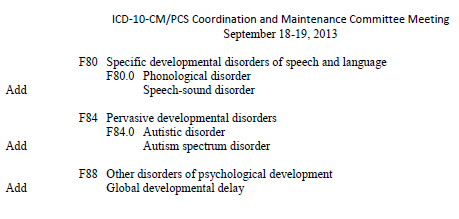
But on Pages 45-46, under “Additional Tabular List Inclusion Terms for ICD-10-CM”, a further 17 proposals and changes are listed for consideration for addition to the Mental and behavioral disorders F codes.
These include the addition of the new DSM-5 categories, Somatic symptom disorder (SSD) and Illness anxiety disorder, as inclusion terms, under the ICD-10-CM Somatoform disorders section, thus:
Source: September 2013 Diagnosis Agenda, Page 45
The Diagnosis Agenda can be downloaded here: http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
Q: Is “Somatic symptom disorder” being proposed to replace several existing ICD-10-CM Somatoform disorders categories and is a unique new code proposed to be assigned to SSD?
A: No, not in the proposal as it stands in the Diagnosis Agenda document.
The proposal is to add SSD as an inclusion term under F45.1 Undifferentiated somatoform disorder. This is the ICD-10-CM code to which SSD is cross-walked in the DSM-5.
Illness anxiety disorder is being proposed as an inclusion term under F45.21 Hypochondriasis. This is the ICD-10-CM code to which Illness anxiety disorder is cross-walked in the DSM-5.
Q: What should I include in my objection?
A: Responders are being asked by NCHS/CMS to consider the following: Whether you agree with a proposal, disagree (and why), or have an alternative proposal to suggest.
Responders are also being asked to comment on the timing of those proposals that are being requested for approval for October 2014: Does a specific proposal for a new or changed Index entry and Tabular List entry meet the criteria for consideration for implementation during a partial code freeze [6] or should consideration for approval be deferred to October 2015?
And separately, and where applicable, comment on the creation of a specific new code for the condition effective from October 1, 2015. (This is not applicable in the case of SSD or Illness anxiety disorder.)
• Since no timing has been specified for the proposed insertion of the requests on Pages 45-46, I suggest stating that as a poorly validated disorder construct, SSD does not meet NCHS/CMS criteria for “new diseases/new technology procedures, and any minor revisions to correct reported errors in these classifications” and should not be considered for approval during a partial code freeze.
+++
On Day Two of the meeting, APA’s Darrel Regier presented 7 proposals for additions or changes, discussed APA’s rationales for each of these requests, in turn, and fielded any resulting questions or comments from the floor or from the meeting chairpersons.
Rationales, references, specific coding proposals for addition as inclusion terms in October 2014 (and subsequent code modifications in those cases where a unique new ICD code is proposed to be created for the term effective from October 2015) are also set out in the Agenda document (from Page 32).
But there was no presentation on behalf of APA, or by representatives of NCHS or CMS, or by anyone else for the specific proposal to add Somatic symptom disorder (SSD) and Illness anxiety disorder as inclusion terms under the ICD-10-CM Somatoform disorders.
No rationales for their inclusion or references to scientific evidence to support the validity of these new DSM-5 constructs have been published in the Diagnosis Agenda and there was no discussion of these two proposals during the course of the meeting.
The requesters of the proposals set out on Pages 45-46 are not identified, so it is unclear whether these “Additional Tabular List Inclusion Terms” are being proposed by APA or by NCHS/CMS.
• I suggest you comment in submissions on the absence from both the Agenda document and the meeting presentations of rationales and references to enable proper public scrutiny, consideration and informed responses to the proposed inclusion of these two terms.
All that was said about the list of proposals on Pages 45-46 was the following, after Dr Regier had wrapped up his own presentation and handed the podium back to the Co-Chair:
[Unofficial transcription from videocast] Donna Pickett (CDC):
• You might also consider quoting the APA’s disturbing DSM-5 field trial data (see March 2013 BMJ commentary by Prof Allen Frances for data).
• Or quote the SSD work group’s recognition of the shaky foundations and lack of scientific robustness for its new DSM-5 construct:
In its recent paper: Somatic Symptom Disorder: An important change in DSM, the SSD work group acknowledges the “small amount of validity data concerning SSD” and that much “remains to be determined” about the utility and reliability of the specific SSD criteria and its thresholds when applied in busy, general clinical practice, and there are “vital questions that must be answered.” [7]
• There is no body of published research on the epidemiology, clinical characteristics or treatment of the APA’s Somatic symptom disorder construct.
• There is a paucity of rigorous evidence for the validity, safety, reliability, acceptability and utility of the SSD construct when applied to adults and children in diverse clinical settings and across a spectrum of health and allied professionals.
• NCHS/CMS has insufficient scientific basis for the approval of SSD as a valid new disorder construct for inclusion within ICD; has published no independent field trial data and provided no rationale to inform public responses.
+++
Why is it important to submit objections?
If SSD is inserted as an inclusion term to an existing code in ICD-10-CM this may leverage the future replacement of several existing ICD-10-CM Somatoform disorders categories with the SSD construct, to more closely mirror DSM-5.
Inserting SSD as an inclusion term into ICD-10-CM may make it easier for ICD-11 to justify its proposal for a Bodily distress disorder to replace several existing ICD-10 Somatoform disorders categories. Though BDD may not mirror SSD exactly, it is anticipated to incorporate SSD’s characteristics and thereby facilitate harmonization between ICD-11 and DSM-5 disorder terminology.
As set out many times during the three DSM-5 stakeholder reviews and in several papers published earlier this year with Prof Allen Frances, DSM-5 SSD has highly subjective and loose, easily met criteria.
A mental health diagnosis of SSD can be applied as a “bolt-on” to any chronic medical diagnosis – to patients with cancer, diabetes, heart disease, MS, angina, ME and CFS, IBS, FM, chronic pain conditions. It can be applied to adults and children (or to the caregivers of children with chronic illnesses).
SSD may become the dustbin diagnosis into which those with persistent, “medically unexplained” somatic (bodily) symptoms will be shovelled. Patients with rare or hard to diagnose illnesses may find themselves mislabelled with SSD.
Implications for the potential impact on patients for an additional diagnosis of SSD are set out (about half way down the page) in my report Somatic Symptom Disorder could capture millions more under mental health diagnosis and in copies of submissions to the three DSM-5 stakeholder review periods, collated on this site.
Also in Mary Dimmock’s 2012 SSD Call to Action materials.
There is a now a copy of the 20 March, 2013 BMJ commentary “The new somatic symptom disorder in DSM-5 risks mislabeling many people as mentally ill” by Prof Allen Frances (with Suzy Chapman) on the NAPPS Skills (Northern Association for Persistent Physical Symptoms) site (Vincent Deary’s group) in this PDF.
If you’ve not already done so, please get an objection in before November 15.
And please alert all contacts, advocates, patient groups and professionals to the November 15 deadline and the need for input and objections.
Further information:
1 Crazy Like Us: How the U.S. Exports Its Models of Illness – DSM-5 is Americanizing the world’s understanding of the mind Christopher Lane, Ph.D. in Side Effects, October 9, 2013
2. Dx Revision Watch: APA petitions CMS for additions to ICD-10-CM: Deadline for public comment and objections November 15: http://wp.me/pKrrB-3tq
3. Dx Revision Watch: Videos and meeting materials: September 18- 19 ICD-9-CM Coordination and Maintenance Committee meeting: http://wp.me/pKrrB-3tV
4. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1757346
5. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013
September C & M meeting Diagnosis Agenda Proposals PDF document [PDF – 342 KB]
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
6. Partial Freeze of Revisions to ICD-9-CM and ICD-10-CM/PCS
7. Somatic Symptom Disorder: An important change in DSM. Dimsdale JE, Creed F, Escobar J, Sharpe M, Wulsin L, Barsky A, Lee S, Irwin MR, Levenson J. J Psychosom Res. 2013 Sep;75(3):223-8. Epub 2013 Jul 25.
Share this:
Filed under American Psychiatric Association (APA), Bodily Distress Disorders, CMS, Criticism of DSM-V, DSM-5, Diagnostic classification, DSM-5, ICD-10-CM, ICD-11, Somatic Symptom Disorder, Somatoform Disorders Tagged with american psychiatric association, dsm-5, functional somatic syndrome, icd-10-cm, icd-11, institute of psychiatry, NCHS, public comment, somatic symptom disorder, somatoform disorders