National Institute of Mental Health (NIMH) to ditch the DSM
Post #241 Shortlink: http://wp.me/pKrrB-2UL
An edited version of the post published on May 3
 NIMH to ditch DSM
NIMH to ditch DSM
Earlier this week, in a blog dated April 29, Thomas Insel, National Institute of Mental Health’s Director, quietly drove another nail into the coffin of DSM-5.
NIMH, part funders of the 13 DSM-5 Research Planning Conferences held between 2004 and 2008 and the monographs that resulted out of them, announced that NIMH “will be re-orienting its research away from DSM categories.”
I don’t have figures for how much funding NIMH has sunk into the development of DSM-5.
This announcement comes just three weeks before the American Psychiatric Association launches its next edition of the Diagnostic and Statistical Manual of Mental Disorders, with a clutch of spin off publications scheduled for release in May and September.
APA has yet to issue a statement or comment in the press.
At the end of this post are links to the NIMH Research Domain Criteria (RDoC) posted in 2011, and a commentary by James Phillips, MD, for Psychiatric Times, from April 2011: “DSM-5 and the NIMH Research Domain Criteria Project.”
You can read Thomas Insel’s announcement in full, below, followed by a round up of media coverage.
Additional coverage and commentary is being added, as it comes in, below the NIMH announcement in the pale blue box.
Most recently added: Dr Tad; Neurocritic BlogSpot
+++
On April 24, in Mental health: On the spectrum, Nature had reported:
“Research suggests that mental illnesses lie along a spectrum — but the field’s latest diagnostic manual still splits them apart…
“…The APA claims that the final version of DSM-5 is a significant advance on the previous edition and that it uses a combination of category and dimensional diagnoses. The previously separate categories of substance abuse and substance dependence are merged into the new diagnosis of substance-use disorder. Asperger’s syndrome is bundled together with a handful of related conditions into the new category called autism-spectrum disorder; and OCD, compulsive hair-pulling and other similar disorders are grouped together in an obsessive–compulsive and related disorders category. These last two changes, Regier says, should help research scientists who want to look at links between conditions. “That probably won’t make much difference to treatment but it should facilitate research into common vulnerabilities,” he says.
“The Research Domain Criteria project is the biggest of these research efforts. Last year, the NIMH approved seven studies, worth a combined US$5 million, for inclusion in the project — and, Cuthbert says, the initiative “will represent an increasing proportion of the NIMH’s translational-research portfolio in years to come”. The goal is to find new dimensional variables and assess their clinical value, information that could feed into a future DSM.
“One of the NIMH-funded projects, led by Jerzy Bodurka at the Laureate Institute for Brain Research in Tulsa, Oklahoma, is examining anhedonia, the inability to take pleasure from activities such as exercise, sex or socializing. It is found in many mental illnesses, including depression and schizophrenia.
“Bodurka’s group is studying the idea that dysfunctional brain circuits trigger the release of inflammatory cytokines and that these drive anhedonia by suppressing motivation and pleasure. The scientists plan to probe these links using analyses of gene expression and brain scans. In theory, if this or other mechanisms of anhedonia could be identified, patients could be tested for them and treated, whether they have a DSM diagnosis or not.
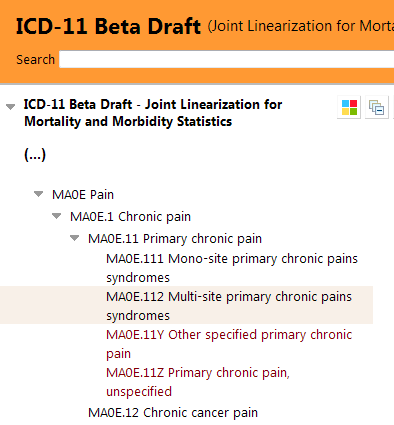
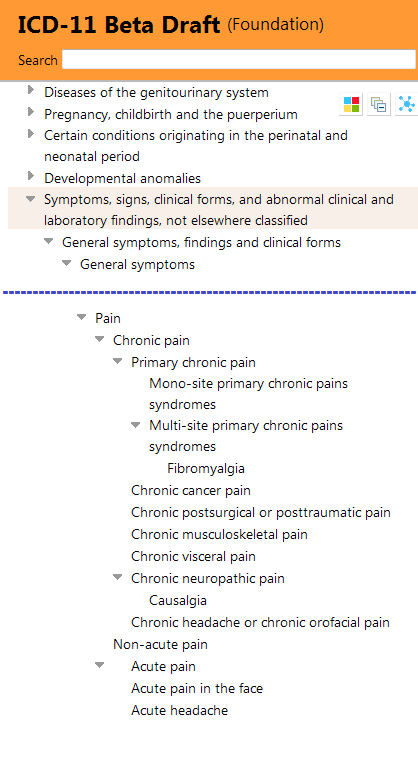
“One of the big challenges, Cuthbert says, is to get the drug regulators on board with the idea that the DSM categories are not the only way to prove the efficacy of a medicine. Early talks about the principle have been positive, he says. And there are precedents: “Pain is not a disorder and yet the FDA gives licences for anti-pain drugs,” Cuthbert says.
“Going back to the drawing board makes sense for the scientists, but where does it leave DSM-5? On the question of dimensionality, most outsiders see it as largely the same as DSM-IV. Kupfer and Regier say that much of the work on dimensionality that did not make the final cut is included in the section of the manual intended to provoke further discussion and research. DSM-5 is intended to be a “living document” that can be updated online much more frequently than in the past, Kupfer adds. That’s the reason for the suffix switch from V to 5; what comes out next month is really DSM-5.0. Once the evidence base strengthens, he says, perhaps as a direct result of the NIMH project, dimensional approaches can be included in a DSM-5.1 or DSM-5.2…”
National Institute of Mental Health (NIMH) announcement
Transforming Diagnosis
By Thomas Insel on April 29, 2013
Thomas R. Insel, M.D., is Director of the National Institute of Mental Health (NIMH).
“…Patients with mental disorders deserve better. NIMH has launched the Research Domain Criteria (RDoC) project to transform diagnosis by incorporating genetics, imaging, cognitive science, and other levels of information to lay the foundation for a new classification system…”
“…That is why NIMH will be re-orienting its research away from DSM categories. Going forward, we will be supporting research projects that look across current categories – or sub-divide current categories – to begin to develop a better system….”
+++
Dr Tad Blog
Paradigms lost: NIMH, McGorry & DSM-5’s failure
Dr Tad | May 4, 2013
Neurocritic Blogspot
RDoC Dimensional Approach for Research vs. DSM-5 for Diagnosis
Neurocritic | May 5, 2013
Article in Romanian
DESCOPERĂ
Cea mai importantă ştiinţă a minţii umane, psihiatria, se transformă în urma unei decizii importante
Article in French
Psychomédia
Le National Institute of Mental Health (NIMH) américain se distance du DSM-5 de l’American Psychiatric Association
Soumis par Gestion le 3 mai 2013
“Le National Institute of Mental Health (NIMH) américain réoriente ses recherches en se distançant du DSM, le Diagnostic and Statistical Manual of Mental Disorders, dont la cinquième édition sera lancée par l’American Psychiatric Association le 22 mai, explique son directeur, Thomas Insel, dans un billet publié le 29 avril…”
Article in Turkish
Psikiyatristler DSM tanı kriterlerini terk ediyor!
Dünyadaki en büyük ruh sağlığı araştırma kurumlarından ABD Ulusal Sağlık Kurumu (NIMH), psikiyatrik rahatsızlıkların semptomlara bağlı olarak belirlenmesine dayanan tanı yöntemini terk ediyor.
Pazar, 05 Mayıs 2013
Scientific American John Horgan Blog
Psychiatry in Crisis! Mental Health Director Rejects Psychiatric “Bible” and Replaces With… Nothing
“NIMH director Insel doesn’t mention it, but I bet his DSM decision is related to the big new Brain Initiative, to which Obama has pledged $100 million next year.”
John Horgan | May 4, 2013
Psychology Today
Side Effects | Christopher Lane Ph.D.
The NIMH Withdraws Support for DSM-5
The latest development is a humiliating blow to the APA.
Christopher Lane, Ph.D. | May 4, 2013
Government Health IT
NIMH moving beyond DSM
Anthony Brino, Associate Editor | May 3, 2013
1 Boring Old Man
old news…
1 Boring Old Man | May 3, 2013
Previously posted
Mindhacks blog
National Institute of Mental Health abandoning the DSM
“In a potentially seismic move, the National Institute of Mental Health – the world’s biggest mental health research funder, has announced only two weeks before the launch of the DSM-5 diagnostic manual that it will be “re-orienting its research away from DSM categories”.
In the announcement, NIMH Director Thomas Insel says the DSM lacks validity and that “patients with mental disorders deserve better”.
This is something that will make very uncomfortable reading for the American Psychiatric Association as they trumpet what they claim is the ‘future of psychiatric diagnosis’ only two weeks before it hits the shelves.
As a result the NIMH will now be preferentially funding research that does not stick to DSM categories…”
New Scientist
Psychiatry divided as mental health ‘bible’ denounced
Andy Coghlan and Sara Reardon | May 3, 2013
“The world’s biggest mental health research institute is abandoning the new version of psychiatry’s “bible” – the Diagnostic and Statistical Manual of Mental Disorders, questioning its validity and stating that “patients with mental disorders deserve better”. This bombshell comes just weeks before the publication of the fifth revision of the manual, called DSM-5…”
“…We cannot succeed if we use DSM categories as the gold standard,” says Insel. “That is why NIMH will be reorienting its research away from DSM categories,” says Insel. Prominent psychiatrists contacted by New Scientist broadly support Insel’s bold initiative. However, they say that given the time it will take to realise Insel’s vision, diagnosis and treatment will continue to be based on symptoms.
“Insel is aware that what he is suggesting will take time – probably at least a decade, but sees it as the first step towards delivering the “precision medicine” that he says has transformed cancer diagnosis and treatment. “It’s potentially game-changing, but needs to be based on underlying science that is reliable,” says Simon Wessely of the Institute of Psychiatry at King’s College London. “It’s for the future, rather than for now, but anything that improves understanding of the etiology and genetics of disease is going to be better [than symptom-based diagnosis].”
New Scientist opinion piece
One manual shouldn’t dictate US mental health research
“The new edition of the DSM “bible” is so flawed that the US National Institute of Mental Health is right to abandon it, says Allen Frances”
Allen Frances, MD | May 3, 2013
@AllenFrancesMD on Twitter
@AllenFrancesMD: @dxrevisionwatch Hype alert. The NIMH dx approach is a necessary, but guarantees nothing in the future and offers nothing in the present.
The Verge
Federal institute for mental health abandons controversial ‘bible’ of psychiatry
Katie Drummond | May 3, 2013
“In a surprising move, the US government institute responsible for overseeing mental health research is distancing itself from the Diagnostic and Statistical Manual of Mental Disorders, or DSM. The DSM has, for several decades, been perceived as the “bible” that delegates how psychiatric illnesses are defined, diagnosed, and treated.”
“The National Institute of Mental Health (NIMH) — which funds more research into mental illness than any other agency in the world — this week announced a plan to re-orient its investigations “away from DSM categories.” The move comes mere weeks before the publication of the DSM-5, an update to the manual that’s been mired in controversy because of several contentious changes to existing diagnostic criteria…”
CBS News
National Institute of Mental Health no longer will use DSM diagnoses in studies
Stephanie Pappas | Livescience.com | May 3, 2013
Pharmalive
NIMH Director Says The Bible Of Psychiatry Lacks Validity
Ed Silverman | May 3, 2013
MIT Technology Review
NIMH Will Drop Widely Used Psychiatry Manual
Susan Young | May 3, 2013
Science 2.0
NIMH Delivers A Kill Shot To DSM-5
By Hank Campbell | May 3, 2013
Pacific Standard [Not on NIMH announcement]
Psychiatry’s Contested Bible: How the New DSM Treats Addiction
The 1,000-page psychiatrists’ Big Book will redefine addiction. Critics are already demanding a boycott.
Michael Dhar | May 3, 2013
Drug Rehab [Not on NIMH announcement]
Somatic Symptom Disorder
drugrehab in Mental Health | April 30, 2013
+++
+++