New Danish and German guidelines for “Bodily distress” and “functional disorders”
+++
Related information:
Trygfonden invites applications for funding for research on functional disorders
Trygfonden has allocated 48 million for research on functional disorders. The application deadline for the last 28 million kroner is 6 April 2010.
Lene Toscano gets 3.3 million kr. for dissemination of knowledge about functional disorders
Specialist in General Medicine Lene Toscano, Aarhus University Hospital, has received 3,336,458 kr. from TrygFonden to examine how best to communicate and share knowledge about functional disorders.
+++
As previously posted:
In February, I published information on the status of current proposals for revision of ICD-10 “Somatoform Disorders” for the ICD-11 core version, as displayed in the ICD-11 Beta drafting platform, and on proposals for ICD-11-PHC, the abridged primary care version of ICD.
In Part Two of that post, I compiled information on “Bodily Distress Syndrome,” a disorder construct developed by Per Fink and colleagues initially for research studies, now used in clinical practice at The Research Clinic for Functional Disorders and Psychosomatics, Aarhus.
See post #222 ICD-11 Beta draft and Bodily Distress Disorders; Per Fink and Bodily Distress Syndrome Parts One and Two
+++
Today, I have three new “Bodily Distress Disorders” related items to bring to your attention:
1. The World Psychiatric Association (WPA) is holding its 2013 International Congress in October, in Vienna. Four topics relating to “Bodily Distress Disorders” are being presented:
Bodily Distress Disorders and the new classifications
Bodily Distress Disorders at the work place: prevention and treatment
A stepped care approach for bodily distress disorders: the new interdisciplinary German guideline
Raising the awareness for the health political relevance of Bodily Distress Disorders – a European agenda
Symposia presenters include:
Francis Creed (member of the DSM-5 Somatic Symptom Disorders Work; member of the WHO Working Group on Somatic Distress and Dissociative Disorders, reporting to the International Advisory Group for the Revision of ICD-10 Mental and Behavioural Disorders; co-author book [1], paper [2]).
Per Fink (The Research Clinic for Functional Disorders and Psychosomatics, Aarhus, Denmark, co-author book [1], paper [3]).
Peter Henningsen (Co-author book [1]).
2] A new German guideline has been published, with summary texts in German and English language:
Neue Leitlinien zu funktionellen und somatoformen Störungen
CLINICAL PRACTICE GUIDELINE Non-Specific, Functional, and Somatoform Bodily Complaints
Rainer Schaefert, Constanze Hausteiner-Wiehle, Winfried Häuser, Joram Ronel, Markus Herrmann, Peter Henningsen. Dtsch Arztebl Int 2012; 109(47): 803−13 [PMID 23341111]
Abstract [in English] here:
New guidelines on functional and somatoform disorders
The S3 guideline “Dealing with patients with non-specific, functional and somatoform bodily symptoms” emphasizes the similarities in the management of the manifold manifestations of so called “medically unexplained symptoms” and gives recommendations for a stepped and collaborative diagnostic and therapeutic approach in all subspecialties and all levels of health care. It has a special focus on recommendations regarding attitude, physician-patient-relationship, communication, the parallelization of somatic and psychosocial diagnostics and a stepped therapeutic approach. The “Evidence-based guideline psychotherapy in somatoform disorders and associated syndromes” provides a differentiated analysis of the current evidence regarding the effectiveness of various psychotherapeutic interventions for the most relevant manifestations of functional and somatoform disorders. In combination, both guidelines pose important advances for treatment quality in Germany, but also illustrate remarkable structural and research deficits.
Abstract [in German] here:
Neue Leitlinien zu funktionellen und somatoformen Störungen
Official summary version texts:
English language version:
or open PDF on Dx Revision Watch:
+++
German language version:
MEDIZIN: Klinische Leitlinie Nicht-spezifische, funktionelle und somatoforme Körperbeschwerden
Clinical Practice Guideline: Non-specific, functional and somatoform bodily complaints
Dtsch Arztebl Int 2012; 109(47): 803-13; DOI: 10.3238/arztebl.2012.0803
or open PDF on Dx Revision Watch:
Correspondence in response to summary version:
In Reply:
Dr. med. Rainer Schaefert
Klinik für Allgemeine Innere Medizin und Psychosomatik, Universitätsklinikum Heidelberg
3] New Danish Association for General Practitioners (DSMA) guide for general practice on functional disorders:
Funktionelle lidelser for Almen Praksis
Ny vejledning sætter fokus på funktionelle lidelser Practicus | April 2013
“New guide focuses on functional disorders”
[Article in Danish]
This article introduces the new Danish Association for General Practitioners (DSMA) guide for general practitioners, published this May. The Working Group for the guide, which included Per Fink, was chaired by Marianne Rosendal.
Access document here in PDF [in Danish]:
Funktionelle lidelser Dansk Selskab for Almen Medicin 2013
or open PDF on Dx Revision Watch: Funktionelle lidelser 2013
Related information:
Lene Toscano gets 3.3 million kr. for dissemination of knowledge about functional disorders
Specialist in General Medicine Lene Toscano, Aarhus University Hospital, has received 3,336,458 kr. from TrygFonden to examine how best to communicate and share knowledge about functional disorders.
Notes:
ICD-11 Beta drafting platform Bodily Distress Disorder: Mild; Moderate; Severe
“Bodily distress disorder” (BDD) is being proposed as a new category for ICD-11 to replace a number of existing ICD-10 “Somatoform Disorders.”
An alternative construct, called Bodily stress syndrome (BSS), has been put out for international primary care focus group evaluation by the working group for the revision of ICD-10-PHC (the abridged primary care version of ICD-10), and will be undergoing ICD-11 field testing and analysis. There is no public domain information available on where BSS will be field tested or on field trial study design, patient selection, criteria etc.
Although ICD-11 is at the Beta drafting stage and scheduled for WHA approval in 2015, the public version of the Beta drafting platform has yet to define this proposed new BDD category, characterize its three, proposed severities: Mild; Moderate; Severe, or populate any of its “Content Model” parameters.
It has sat there since February 2012, a tabula rasa.
At the time of writing, it remains unspecified which disorders BDD is proposed to capture.
It isn’t clear whether its criteria are proposed to be based on unspecified somatic symptoms, symptom counts or specific constellations of symptoms (eg gastrointestinal, musculoskeletal); whether psychological or behavioural responses are central to its definition; whether it is intended to be inclusive of selected of the so-called “functional somatic syndromes”; whether, like DSM-5’s SSD, its reach would be extended to include patients with somatic symptoms in association with diagnosed diseases, such as cancer or diabetes.
It is not possible to determine from what little information displays in the public version of the drafting platform whether ICD-11 proposes that BDD would mirror or incorporate Per Fink’s construct of “Bodily Distress Syndrome” for definition, criteria, severity specifiers, inclusions, exclusions etc; or whether it intends BDD to also incorporate DSM-5’s “Somatic Symptom Disorder” (and if so, how might this be achieved, since BDS and SSD lack congruency); or whether a unique definition for BDD is being developed and tested specifically for ICD-11.
Until ICD-11 defines BDD, it presents barriers to professional and lay stakeholders inputting meaningful comment on this proposal, which has remained undefined for over a year.
If the working groups advising ICD-11 Revision are putting forward a Per Fink “BDS” model for BDD, or an adaptation of Per Fink’s model, it is not known how WHO classification experts view any proposal that might seek to shift several, discrete, ICD-10 categories with long-standing classification locations outside the Mental and behavioural disorders chapter of ICD, into Chapter 5, and subsume them under a new disorder construct, for which there is no body of evidence for its validity as a construct and safety of application outside research settings.
Note that the ICD-11 Beta draft is a work in progress: proposals for new disorders for ICD-11 are subject to field trial evaluation and approval by Topic Advisory Group Managing Editors, the ICD-11 Revision Steering Group and WHO classification experts.
These two papers and a book chapter discuss emerging proposals for ICD-11 and ICD-11-PHC:
Lam TP, Goldberg DP, Dowell AC, Fortes S, Mbatia JK, Minhas FA, Klinkman MS. Proposed new diagnoses of anxious depression and bodily stress syndrome in ICD-11-PHC: an international focus group study. Fam Pract 2012 [PMID: 22843638]*
Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry 2012;24:556-67. [PMID: 23244611]
Goldberg DP. Comparison Between ICD and DSM Diagnostic Systems for Mental Disorders. In: Sorel E, (Ed.) 21st Century Global Mental Health. Jones & Bartlett Learning, 2012: 37-53 [Free PDF, Sample Chapter Two: http://samples.jbpub.com/9781449627874/Chapter2.pdf]
*SHORT REPORT Kuruvilla, A, Jacob KS. Perceptions about anxiety, depression and somatization in general medical settings: A qualitative study. National Medical Journal of India, vol. 25, no. 6, pp. 332–335, 2012
+++
What is “Bodily Distress Syndrome”?
The Per Fink et al construct of BDS is a unifying diagnosis that encompasses a group of what are considered to be closely related conditions such as somatization disorder, fibromyalgia, chronic pain disorder, irritable bowel syndrome, chronic fatigue syndrome and ME, multiple chemical sensitivity (MCS) and whiplash associated disorder. On some BDS presentation slides, “Stress and burn out…and many more…” are added to the list.
From the Aarhus Research Clinic website:
“…recent research suggests that the different diagnoses are all subcategories of one single illness, namely BDS…
“…BDS is a new research diagnosis and therefore unfamiliar to many doctors. Most doctors do know the different diagnoses mentioned in the above box, but they are unaware that they can be viewed as one single illness…”
In May 2010, Per Fink and Andreas Schröder, PhD, MD, Aarhus Universitetshospital, Denmark, published the paper, “One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders.” [Abstract: PMID: 20403500].
According to the authors of this 2012 EACLPP Conference Abstract: Bodily Distress Syndrome: A new diagnosis for functional disorders in primary care, the concept of “Bodily Distress Syndrome”
is expected to be integrated into the upcoming versions of classification systems.
This 2010 Danish journal article sets out proposals by Fink et al for a new classification:
Journal article: Fink P, Rosendal, M et al. Ny fælles diagnose for de funktionelle sygdomme. [PDF, in Danish]
Note: This proposal by Fink, Rosendal et al has three hitherto discrete ICD-10 classifications, Fibromyalgia (M79.7), IBS (K58) and Chronic Fatigue Syndrome (indexed to G93.3 in ICD-10; classified in ICD-11 Beta draft as an ICD Title term within ICD-11 Chapter 6: Diseases of the nervous system) proposed to be relocated under the ICD-11 mental and behavioural disorders chapter (Chapter 5) and subsumed under a single new disorder classification, “Bodily Distress Syndrome,” along with Neurasthenia (F48.0), Hypochondriasis and some other ICD-10/DSM-IV Somatoform Disorders.
Page 1837
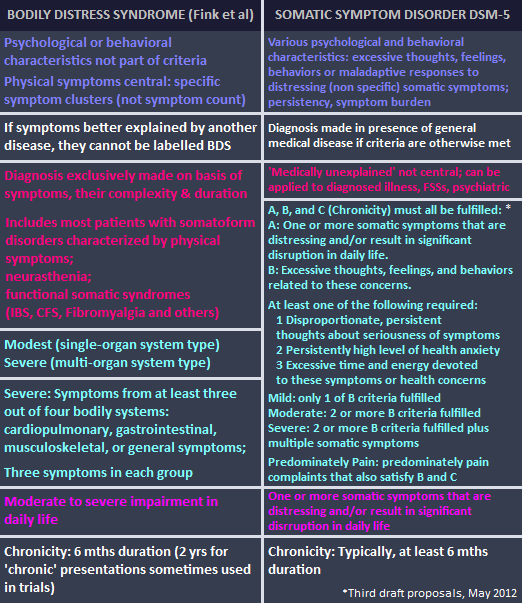
Proposed new classification on left; Current classifications on right:

Here, the same proposal set out in English, from a Danish presentation:
(Note: MS type = Musculoskeletal)
Slide Presentation Two [PDF, in Danish; some slides in English]
Bodily Distress Syndrome (BDS), og helbredsangst Udvikling af diagnoserne, assessment og forskning på området, Oplæg ved Sundhedspsykologisk, Årsmøde 2011
Slide #11 of 97

For further information on proposals for “Bodily Distress Disorder” for ICD-11 and on Per Fink’s “Bodily Distress Syndrome” see Dx Revision Watch post #222: ICD-11 Beta draft and Bodily Distress Disorders; Per Fink and Bodily Distress Syndrome Parts One and Two
References
1. Medically Unexplained Symptoms, Somatisation and Bodily Distress: Developing Better Clinical Services. Creed, Francis; Henningsen, Peter; Fink, Per, Cambridge University Press, 2011. Sample pages on Google Books
2. Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry 2012;24:556-67. [Abstract: PMID: 23244611]
3. Fink P, Schröder A. One single diagnosis, bodily distress syndrome, succeeded to capture 10 diagnostic categories of functional somatic syndromes and somatoform disorders. J Psychosom Res. 2010 May;68(5):415-26. [Abstract: PMID: 20403500]
 WHO-IUPsyS ICD Survey Report Report 2012
WHO-IUPsyS ICD Survey Report Report 2012 2013 All rights reserved. Current Biology,
2013 All rights reserved. Current Biology, 


{kind=link}