Reminder: Next meeting of ICD-10-CM/PCS Coordination and Maintenance Committee: March 19-20, 2014
January 24, 2014
Post #290 Shortlink: http://wp.me/pKrrB-3F1
Update at February 15, 2014:
Tentative diagnosis agenda posted for March 19–20, 2014 meeting on CDC site:
This list of tentative diagnosis agenda topics is not final. The final topics material will be available electronically from the NCHS web site prior to the meeting.
If you are unable to attend the meeting in person there will be conference lines available on the day of the meeting. Individuals do not need to register on line for the meeting if planning to dial in.
NCHS/CMS will be broadcasting the meeting live via Webcast at: http://www.cms.gov/live/
The next meeting of the ICD-10-CM/PCS Coordination and Maintenance Committee is scheduled for March 19–20, 2014. If you are planning to attend the meeting in person you will need to register, online, by March 14.
ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
Public forum to discuss proposed changes to ICD-10-CM and ICD-10-PCS
Wednesday, March 19, 2014 – Thursday, March 2o, 2014
CMS Auditorium, Baltimore, MD
Agendas for the meeting will be posted in February 2014.
If phone lines and live webinar are made available the information will be posted closer to the meeting date.
Day One | Time: 03/19/2014 9:00 AM – 5:00 PM CMS Auditorium
Session: ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
The first day of the meeting, March 19, 2014, will be devoted to procedure code issues.Day Two | Time: 03/20/2014 9:00 AM – 5:00 PM CMS Auditorium
Session: ICD-10-CM/PCS Coordination and Maintenance Committee Meeting
The second day of the meeting, March 20, 2014 will be devoted to diagnosis code topics.
The National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS) are the U.S. governmental agencies responsible for overseeing all changes and modifications to the ICD-9-CM and draft ICD-10-CM/PCS.
NCHS is also responsible for the development of ICD-10-CM, adapted from the WHO’s ICD-10 for U.S. specific use.
The 2014 release of the draft ICD-10-CM (which replaces the July 2013 release) can be viewed or downloaded here.
ICD-10-CM is scheduled for implementation on October 1, 2014. Until that time the codes in ICD-10-CM are not valid for any purpose or use.
New concepts are added to ICD-10-CM based on the established update process for ICD-9-CM (the ICD-9-CM Coordination and Maintenance Committee) and the World Health Organization’s ICD-10 (the Update and Revision Committee).
Meetings of the Coordination and Maintenance Committee are co-chaired by a representative from NCHS and from CMS. Responsibility for maintenance of the ICD-9-CM is divided between these two agencies, with classification of diagnoses by NCHS and procedures by CMS.
The name of the Committee will change to the ICD-10-CM/PCS Coordination and Maintenance Committee with the March meeting, as the last updates to ICD-9-CM/PCS took place on October 1, 2013.
Meetings are held twice yearly, in public, at CMS headquarters in Baltimore, MD. The next meeting is scheduled for March 19–20, 2014. The fall meeting is scheduled for September 23–24, 2014.
Coordination and Maintenance Committee
The Committee provides a public forum to discuss proposed modifications, code changes, updates and corrections to the diagnosis codes in ICD-10-CM and procedural codes in ICD-10-PCS.
Public participation can also take place via phone conference link and live webinar. (Details for both in the Agenda documents.)
Agendas are posted approximately one month prior to the meetings. Diagnostic and procedural proposal Topic Packets, meeting materials, hand outs and presentation slides are posted on the CDC and CMS websites shortly before a meeting.
Up until 2011, transcripts of meeting proceedings were provided. Provision of transcripts is now replaced with videocasts for the full, two-day proceedings, available from the CMS website and posted on YouTube, and a brief Meeting Summary report, available from the CDC site shortly after the meeting.
For attendance in person, prior registration is required, via the CMS meeting registration website. Registration opens approximately one month prior to a meeting and closes a few days before Day One of a meeting.
Proposals for modifications, additions, corrections
Suggestions for modifications to ICD-10-CM/PCS come from both the public and private sectors. Since the draft ICD-10-CM is adapted from the WHO’s ICD-10, which is subject to an annual update process, some proposed modifications to ICD-10-CM may reflect updates to the ICD-10.
Interested parties (requestors) must submit proposals for modifications prior to a scheduled meeting and by a specific date. Proposals should be consistent with the structure and conventions of the classification. See Submission of Proposals for submission requirements and proposal samples.
Once proposals have been reviewed, requestors are contacted as to whether their proposal has been approved for presentation at the next Coordination and Maintenance Committee meeting or not.
Approved proposals are presented at the meetings by representatives for professional bodies, advocacy organizations, clinicians, other professional stakeholders or members of the public with an interest, or are sometimes presented by an NCHS/CMS representative on behalf of a requestor.
No decisions on proposed modifications are made at the meetings. Recommendations and comments are reviewed and evaluated, once the comment period has closed, before final decisions are made.
The Coordination and Maintenance Committee’s role is advisory. All final decisions are made by the Director of NCHS and Administrator of CMS.
Final decisions are made at the end of the year and become effective October 1 of the following year.
Submitting written comment on proposals presented at meetings
Comments on proposals are invited, at the meeting, at the end of each presentation, or may be submitted in writing following the meeting, during a one to two month duration public comment period.
Addresses for submitting comments are included in the Agenda Topic Packets published before the meetings. NCHS/CMS state that electronic submissions are greatly preferred over snail mail in order to ensure timely receipt of responses.
Partial code freeze and timing of proposals
According to the Summary of Diagnosis Presentations for the September 18–19, 2013 meeting (for which the comment period closed on November 15):
“Except where noted, all topics are being considered for implementation on October 1, 2015. The addenda items are being considered for implementation prior to October 1, 2014.”
(“ICD-10-CM TABULAR OF DISEASES – PROPOSED ADDENDA” Tabular and Index modification proposals are set out on Diagnosis Agenda Pages 60-66.)
Note that some proposals in the Diagnosis Agenda were requested for insertion in October 2014 as Inclusion Terms to existing codes, with new codes proposed to be created for October 2015, notably, the 6 proposals to insert new DSM-5 disorders into ICD-10-CM presented by Darrel Regier, MD, on behalf of the American Psychiatric Association (Diagnosis Agenda Pages 32-44).
Whether the 17 modifications proposed on Pages 45-46 under “Additional Tabular List Inclusion Terms for ICD-10-CM” which were presented en masse by CDC’s, Donna Pickett, (which include the proposals to add the new DSM-5 “Somatic symptom disorder” and “Illness anxiety disorder” as Inclusion Terms to existing ICD-10-CM F45.x codes) are intended for implementation in October 2014 or in October 2015 is not explicit in the Diagnosis Agenda.
For the September 18–19, 2013 meeting, when submitting written comments, responders were asked to consider the following:
Whether they agree with a proposal, disagree (and why), or have an alternative proposal to suggest. But were also invited to comment on the timing of those proposals that were being requested for approval for October 2014:
Does a request for a new diagnosis or procedure code meet the criteria for implementation in October 2014 during a partial code freeze* based on the criteria of the need to capture a new technology or disease; or should consideration for approval be deferred to October 2015? And separately, to comment on the creation of a specific new code for the condition effective from October 1, 2015 (where requested).
Any code requests that do not meet the criteria [for inclusion during a partial freeze] will be evaluated for implementation within ICD-10-CM on and after October 1, 2015 once the partial freeze has ended and regular (at least annual) updates to ICD-10-CM/PCS resume.
*Partial Code Freeze of Revisions to ICD-9-CM and ICD-10-CM/PCS
- October 1, 2011 is the last major update of ICD-9-CM. Any further revisions to ICD-9-CM will only be for a new disease and/or a procedure representing new technology. Revisions will be posted on this website as addenda (revisions to procedures are posted on the CMS website).
- After October 1, 2011 there will be no further release of ICD-9-CM on CD-ROM.
- October 1, 2011 is the last major update of ICD-10-CM/PCS until October 1, 2015.
- Between October 1, 2011 and October 1, 2015 revisions to ICD-10-CM/PCS will be for new diseases/new technology procedures, and any minor revisions to correct reported errors in these classifications.
- Regular (at least annual) updates to ICD-10-CM/PCS will resume on October 1, 2015.
Public comments not made public
Note that written public comments received by NCHS (Diagnosis) and CMS (Procedural) on proposals requested via these meetings are not aggregated and made publicly accessible. Nor are the names of organizations, professional bodies, individuals or others who have submitted comments listed publicly. It is not possible to scrutinize the number, provenance or substance of the comments received in support of, or in opposition to requests for modifications to ICD-10-CM presented via these meetings. Nor are NCHS/CMS’s rationales for the approval or rejection of requests for modifications to diagnosis or procedural codes on public record.
September 18–19, 2013 meeting
A substantial number of modifications were proposed via the September 2013 meeting for both procedural and diagnosis codes. These are set out in the Agenda/Topic Packet PDF documents:
Videocasts for full two day meeting proceedings and Meeting Materials (collated on Dx Revision Watch site)
Summary of Diagnosis Presentations
The ICD-9-CM timeline (for the remainder of its life) and the ICD-10-CM/PCS timeline are set out on Pages 3-8 of the Diagnosis Agenda.
Key dates for the forthcoming March 19–20, 2014 meeting
January 17, 2014: deadline for submitting topics to be discussed at the March 19–20, 2014 ICD-10-CM/PCS Coordination and Maintenance Committee (reached).
February 14: registration for attendance opens.
March 14: deadline for registration.
Go here for registration details. (CMS confirmed to me via email on 01.23.13 that the deadline for registration is March 14, not February 14, as incorrectly published in the Diagnosis Agenda timeline.)
April 18, 2014: deadline for receipt of public comments on proposed codes and modifications tabled for March meeting. (Note there is only a 4 week period following this meeting during which written comments can be submitted.)
Key ICD-10-CM/PCS Timeline dates extracted from full timeline, Pages 3-8, September 18-19, 2013 Diagnosis Agenda
March 19–20, 2014: ICD-10-CM/PCS Coordination and Maintenance Committee meeting.
April 1, 2014: There will be no new ICD-9-CM codes to capture new diseases or technology on April 1, 2014, since the last updates to ICD-9-CM will take place on October 1, 2013.
April 2014: Notice of Proposed Rulemaking to be published in the Federal Register as mandated by Public Law 99-509. This notice will include references to the complete and finalized FY 2015 ICD-10-CM diagnosis and ICD-10-PCS procedure codes. It will also include proposed revisions to the MS-DRG system based on ICD-10-CM/PCS codes on which the public may comment. The proposed rule can be accessed at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html?redirect=/AcuteInpatientPPS/IPPS/list.asp
April 18, 2014: Deadline for receipt of public comments on proposed code [at March meeting.]
June 2014: Final addendum posted on web pages as follows:
Diagnosis addendum – http://www.cdc.gov/nchs/icd/icd10cm.htm
Procedure addendum – http://cms.hhs.gov/Medicare/Coding/ICD10/index.html
September 23–24, 2014: ICD-10-CM/PCS Coordination and Maintenance Committee 2014 meeting.
October 1, 2014: New and revised ICD-10-CM and ICD-10-PCS codes go into effect along with DRG changes. Final addendum posted on web pages as follows:
Diagnosis addendum – http://www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
Procedure addendum – http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/addendum.html
November 2014: Any new ICD-10 codes required to capture new technology that will be implemented on the following April 1 will be announced. Information on any new codes to be implemented April 1, 2015 will be posted on the following websites:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/addendum.html




{kind=link}
Which new DSM-5 disorders proposed for inserting into ICD-10-CM are already added to the ICD-11 Beta draft?
November 6, 2013 by admindxrw
Post #280 Shortlink: http://wp.me/pKrrB-3vs
Update to ICD-11 Beta draft at February 3, 2014:
Since my update on January 3, in the ICD-11 Beta draft, Hypochondriasis (illness anxiety disorder) has since been reverted to Hypochondriasis with illness anxiety disorder listed, instead, as an Inclusion term to Hypochondriasis.
Hypochondriasis was subsequently assigned to three parents:
Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere; Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders;
At February 3, Hypochondriasis has been removed from parent Bodily distress disorders and is currently assigned dual parentage under:
Obsessive-compulsive and related disorders;
Anxiety and fear-related disorders
Foundation View:
hppt://apps.who.int/classifications/icd11/browse/f/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
Joint Linearization for Mortality and Morbidity Statistics View:
http://apps.who.int/classifications/icd11/browse/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f675329566
The Definition for Hypochondriasis currently displaying in the Beta draft appears to be the legacy Definition, unrevised from ICD-10.
Update to ICD-11 Beta draft at January 3, 2014:
Revision to ICD-11 Beta draft: In the report below, I stated:
As the ICD-11 Beta drafting platform now stands, at January 3, 2014, the DSM-5 term “(illness anxiety disorder)” has been removed from the “Hypochondriasis (illness anxiety disorder)” disorder name and the term reverted to Hypochondriasis.
The term “illness anxiety disorder” is now displaying as listed under “Synonyms” to Hypochondriasis in the ICD-11 Beta Foundation View, and listed under “All Index Terms” in the Morbidity Linearization View.
As previously posted on November 6, 2013:
In the previous four posts, I have documented the September 18-19, 2013 meeting of the ICD-9-CM Coordination and Maintenance Committee and reported on American Psychiatric Association (APA) proposals for inserting a number of new DSM-5 terms into the forthcoming US specific ICD-10-CM.
I also set out how public and professional stakeholders can submit comment or objections on any of the proposals requested at this meeting before the November 15 deadline.
At the September meeting, Darrel Regier, MD, APA Director of Research, presented six diagnoses that are new to DSM-5 for inclusion within ICD-10-CM, with proposals for assigning unique new codes to these disorders for October 2015 [1].
Some of the DSM-5 disorders, below, presented for consideration for inclusion in ICD-10-CM are already entered into the ICD-11 Beta drafting platform and in some cases, entered into the draft over a year or more ago.*
Binge eating disorder (BED)
(Rationale: Page 32, Diagnosis Agenda: Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Binge eating disorder (BED) as an inclusion term to F50.8 Other eating disorders.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created for F50.81 Binge eating disorder.
ICD-11 public version Beta draft: Binge eating disorder currently proposed to be coded under Feeding and eating disorders and assigned a unique ICD-11 code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Binge eating disorder.
——————————
Gender Identity Disorder in Adolescence and Adulthood
(Rationale: Page 34, Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: that ICD-10-CM change the code for Gender identity disorder in adolescents and adulthood to F64.0 and that “gender dysphoria in adolescents and adults” is added as an inclusion term for this entry.
Source: September 2013 Diagnosis Agenda, Page 34
[See Page 34 of Diagnosis Agenda for discussion of proposed coding changes.]
——————————
Disruptive mood dysregulation disorder (DMDD)
(Rationale: Page 35, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Disruptive mood dysregulation disorder (DMDD) as an inclusion term under F34.8: Other persistent mood [affective] disorders.
Proposal for ICD-10-CM for October 1, 2015: that unique new codes are created at F34.81 Disruptive mood dysregulation disorder and F34.89 Other specified persistent mood disorders.
ICD-11 public version Beta draft: Disruptive mood dysregulation disorder (DMDD) is not currently listed.
——————————
Social (Pragmatic) Communication Disorder
(Rationale: Page 37, Diagnosis Agenda; Page 6, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Social (Pragmatic) Communication Disorder as an inclusion term under F80.89 Other developmental disorders of speech and language.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F80.82 Social pragmatic communication disorder.
Excludes1: Asperger’s syndrome (F84.5)
Autistic disorder (F84.0)
ICD-11 public version Beta draft: Social (Pragmatic) Communication Disorder is not currently listed.
——————————
Hoarding disorder
(Rationale: Page 39, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Hoarding disorder as an inclusion term to F42 Obsessive Compulsive Disorder.
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.2 for Obsessive Compulsive Disorder and F42.3 for Hoarding Disorder in future revisions. (Ms. Pickett stated that new code proposal starting at F42.2 is due to F42.0 and F42.1 deactivation by WHO.)
F42 Obsessive compulsive disorder
New code F42.2 Mixed obsessional thoughts and acts
New code F42.3 Hoarding disorder
New code F42.8 Other obsessive compulsive disorder
New code F42.9 Obsessive-compulsive disorder, unspecified
ICD-11 public version Beta draft: Hoarding disorder currently proposed to be coded under parent Obsessive-compulsive and related disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Hoarding disorder.
——————————
Excoriation (skin picking) disorder
(APA Rationale: Page 41, Diagnosis Agenda, Page 7, Diagnosis Presentations Summary)
Proposal for ICD-10-CM for October 1, 2014: add Excoriation (skin-picking) disorder as an inclusion term to L98.1 Factitial dermatitis (Dermatology section).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created at F42 for F42.4 Excoriation (skin-picking) disorder.
Excludes1: Factitial dermatitis (L98.1)
Other specified behavioral and emotional disorders with onset usually occurring in early childhood and adolescence (F98.8)
ICD-11 public version Beta draft: Excoriation disorder (skin-picking disorder) currently proposed to be coded under Obsessive-compulsive and related disorders under parent Body-focused repetitive behaviour disorders and assigned a unique code. No ICD-11 Definition or other “Content Model” descriptive parameters have yet been populated for Excoriation (skin-picking) disorder.
——————————
Premenstrual dysphoric disorder (PMDD)
(APA Rationale: Page 43, Diagnosis Agenda; Page 7, Diagnosis Presentations Summary)
APA considers that placing PMDD outside the recurrent depressive disorder category is less than optimal for differentiating it from ICD-10-CM N94.3 Premenstrual Tension Syndrome, which is generally less severe than PMDD, and does not require psychiatric treatment. If an alternative code in the F32 series is possible, APA would prefer to modify the code in that section in future revisions.
Proposal for ICD-10-CM for October 1, 2014: add Premenstrual dysphoric disorder as an inclusion term to N94.3 Premenstrual tension syndrome (Chapter 15 Diseases of the genitourinary system).
Proposal for ICD-10-CM for October 1, 2015: that a unique new code is created under Chapter 5 F32.8 Other depressive episodes.
New code F32.81 Premenstrual dysphoric disorder
Excludes1: premenstrual tension syndrome (N94.3)
ICD-11 public version Beta draft: Premenstrual dysphoric disorder (PMDD) currently proposed to be dual coded under Chapter 15 Diseases of the genitourinary system > Premenstrual tension syndrome and also coded under Chapter 5 Depressive disorders and assigned a unique code. A draft ICD-11 Definition has been populated for PMDD but no other ICD-11 “Content Model” descriptive parameters have been populated.
——————————
Somatic symptom disorder and Illness anxiety disorder
Source: September 2013 Diagnosis Agenda, Page 45
Somatic symptom disorder:
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Somatic symptom disorder under F45 Somatoform Disorders as inclusion term to F45.1 Undifferentiated somatoform disorder.
ICD-11 public version Beta draft: There is no Somatic symptom disorder in the ICD-11 Beta draft either as a unique new ICD-11 entity code or as an inclusion term or Synonym to an existing ICD-11 code.
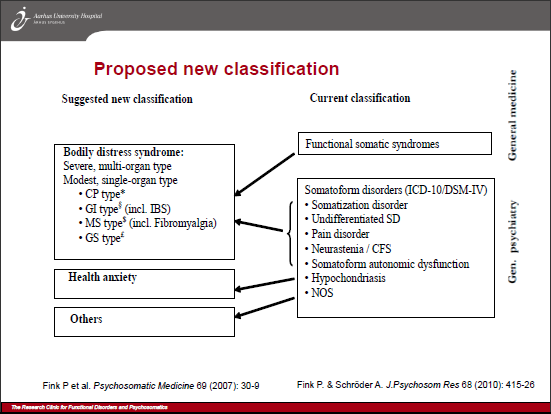
For ICD-11 Core version: the current proposal for the F45 Somatoform disorders is for a proposed new construct, Bodily distress disorder, to replace a number of existing ICD-10 categories under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere. Two specifiers: Bodily distress disorder and Severe Bodily distress disorder have yet to be defined or characterized within the Beta draft and no “Content Model” parameters have yet been populated. ICD-11 plans to field test this proposed new ICD-11 construct.
The Definition for Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere currently displaying in the Beta draft appears to be the legacy Somatoform disorders Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
——————————
Illness anxiety disorder
(No rationale provided: Page 45, Diagnosis Agenda) Requester unspecified
Proposal for ICD-10-CM: add Illness anxiety disorder under F45 Somatoform disorders as inclusion term to F45.21 Hypochondriasis.
ICD-11 public version Beta draft: Illness anxiety disorder is proposed to be dual coded as Hypochondriasis (illness anxiety disorder) under primary parent, Obsessive-compulsive and related disorders and also coded under Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere and assigned a unique code.
The Definition for Hypochondriasis (illness anxiety disorder) currently displaying in the Beta draft appears to be the legacy Definition imported from ICD-10 and does not reflect any proposed structural reorganization or construct revision for the ICD Somatoform disorders categories.
Submitting comments
If you have comments or objections to any of the proposals requested at the September ICD-9-CM C & M Committee meeting, the deadline for submissions is November 15, by email, to Donna Pickett: nchsicd9CM@cdc.gov
+++
References for key documents:
1. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1750103
2. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm#public_meetings
September meeting Proposals [PDF – 342 KB]
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
September meeting Summary of Diagnosis Presentations PDF file [PDF – 347 KB]:
http://www.cdc.gov/nchs/data/icd/icd_summary_sept_181913.pdf
3. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18-19, 2013 meeting materials and four YouTubes of proceedings:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/ICD-9-CM-C-and-M-Meeting-Materials-Items/2013-09-18-MeetingMaterials.html
4. September 19, 2013 Meeting Day Two: ICD-9-CM Coordination and Maintenance Committee Meeting Part 4 videocast:
http://www.youtube.com/watch?v=G-pYdKyr_NE
5. ICD-11 Beta drafting platform (public version):
http://apps.who.int/classifications/icd11/browse/f/en
Share this:
Filed under American Psychiatric Association (APA), CDC, CMS, Criticism of DSM-V, DSM-5, DSM-5, ICD-10-CM, ICD-10-PCS, ICD-11, Somatic Symptom Disorder, WHO (World Health Organization) Tagged with american psychiatric association, binge eating disorder, disruptive mood dysregulation disorder, dsm-5, icd-10-cm, institute of psychiatry, NCHS, premenstrual dysphoric disorder, public comment, somatic symptom disorder