APA petitions CMS for additions to ICD-10-CM: Deadline for public comment and objections November 15
October 8, 2013
Post #276 Shortlink: http://wp.me/pKrrB-3tq
Information in this report relates to American Psychiatric Association (APA) proposals, submitted via the September ICD-9-CM/PCS Coordination and Maintenance Committee Meeting, for the inclusion of a number of additions to the forthcoming US specific ICD-10-CM.
ICD-9-CM is the official system of assigning codes to medical diagnoses in the United States. Next year, ICD-9-CM will be replaced by ICD-10-CM, scheduled for implementation on October 1, 2014.
The DSM is widely used by CMS contractors, federal and state agencies and medical insurers to indicate eligibility for provision of services.
Since the official codes required in the United States for records and reimbursement purposes are ICD-CM codes, DSM diagnoses are cross-walked to the closest approximation of ICD-CM codes to classify diagnoses for insurance claims, research, data capture and other public health purposes.
APA petitions ICD-9-CM Coordination and Maintenance Committee:
The ICD-9-CM and ICD-10-CM coding systems are subject to annual revisions by NCHS and CMS via public review meetings held twice a year (in March and September), followed by brief public comment periods.
October 1, 2011 saw the last major update of ICD-10-CM/PCS until October 1, 2015. Between October 1, 2011 and October 1, 2015 revisions to ICD-10-CM/PCS will be for new diseases/new technology procedures, and any minor revisions to correct reported errors in these classifications. Regular (at least annual) updates to ICD-10-CM/PCS will resume on October 1, 2015.
The ICD-9-CM Coordination and Maintenance Committee will continue to meet twice a year during this partial code freeze. At these meetings, the public will be asked to comment on whether or not requests for new diagnosis or procedure codes should be created based on the criteria of the need to capture a new technology or disease. Any code requests that do not meet the criteria will be evaluated for implementation within ICD-10-CM on and after October 1, 2015 once the partial code freeze has ended.
At last month’s Coordination and Maintenance Committee meeting, APA presented seven diagnoses that are new to DSM-5, along with proposals for new codes for addition to the ICD-10-CM [1]. APA states that the new codes, if approved [by NCHS/CMS], would probably not be added to ICD-10-CM until 2015.
Yesterday, APA published an article in Psychiatric News (the PR organ of the APA), listing the additions and changes proposed by APA via the September meeting (about two thirds into the article):
ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013 DOI: 10.1176/appi.pn.2013.10b30
The following disorders were proposed by APA for inclusion in ICD-10-CM (Pages 32-44, Diagnosis Agenda).
Dr Regier’s presentation starts on Day Two of the meeting, video Part 4, 13:50 mins in from start and concludes after PMDD.
Binge eating disorder (BED);
Disruptive mood dysregulation disorder (DMDD);
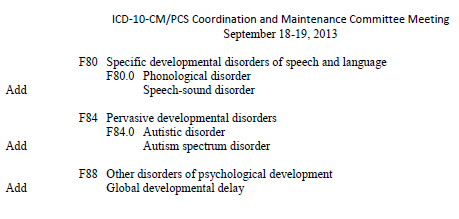
Social (pragmatic) communication disorder;
Hoarding disorder;
Excoriation (skin picking) disorder;
Premenstrual dysphoric disorder (PMDD)
Additionally, the APA has petitioned for revisions to the ICD-10-CM listing for gender dysphoria in adolescents and adults, which is not a new disorder. Dr Regier’s presentation concluded with recommendations for PMDD.
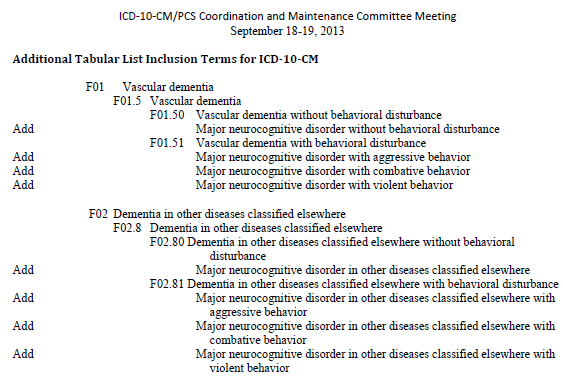
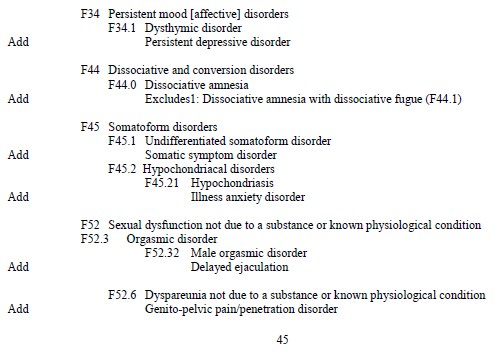
Edit: On Page 45 and 46 of the Agenda, under Additional Tabular List Inclusion Terms for ICD-10-CM a number of other changes to specific Chapter 5 F codes are proposed, including the addition to the ICD-10-CM Chapter 5 codes of the new DSM disorders:
Somatic symptom disorder (proposed as Inclusion term to F45.1 Undifferentiated somatoform disorder)
Illness anxiety disorder (proposed as Inclusion term to F45.21 Hypochondriasis)
None of these 16 proposed additional inclusion terms to the ICD-10-CM Mental and behavioural disorders (Chapter 5) F codes, as listed on Pages 45-46, were presented or discussed by Dr Regier on behalf of the APA but presented briefly and en masse by Donna Pickett.
I have pasted screenshots from the Agenda at the end of this report [Ref 5].
Ms Pickett introduced this section of the Agenda on Day Two, video Part 4, 1 hour 22 mins in from start.
Diagnosis Agenda Item Page 45-46: “Additional Tabular List Inclusion Terms for ICD-10-CM”
Co-Chair Donna Pickett: “…And just to complete the package, there are other Tabular List proposals that appear on Page 45 and 46 that we would also invite your comments on. And again, as with some of the terminology changes that Dr Regier has described the intent here is to make sure that if those terms are being used, that they do have a home somewhere within ICD-10-CM to facilitate people looking these up. So we invite comments. We’re showing the Tabular List proposed changes. However, there obviously would be associated Alphabetic Index changes with that which we didn’t show [in the Agenda] just to keep the package a little bit smaller.”
With no discussion taking place on rationales for individual proposals and no comments or questions being received from the floor or by phone link, Ms Pickett moved swiftly forward to introduce the next Agenda item.
Since these proposals are unattributed in the Agenda, the provenance of these additional 16 code change requests is unclear (that is, whether the requestors are CMS/CDC, Collaborating Centre for the WHO-FIC in North America, WHO ICD-10 Update Committee, WHO ICD-11 Revision, APA or other petitioners).
If the addition of new DSM-5 disorders Somatic symptom disorder and Illness anxiety disorder had been proposed by the APA, it is unclear why these were not included within Dr Regier’s presentation for discussion.
Blink and you might have missed the proposal to incorporate Somatic symptom disorder and Illness anxiety disorder into ICD-10-CM – so little time and attention being devoted to this section of the Agenda.
Note that Hypochondriasis (Illness anxiety disorder) is proposed to be included in the ICD-11 Beta draft under dual parents Obsessive-compulsive and related disorders and Bodily distress disorders, and psychological and behavioural factors associated with disorders or diseases classified elsewhere.
Full proposals from APA and other petitioners can be read in the ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18–19, 2013: Proposals document at:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm
(Diagnosis Agenda) Proposals document [PDF – 342 KB]:
http://www.cdc.gov/nchs/data/icd/icd_topic_packet_sept_181913.pdf
A Summary report of the Procedure part of the September 18–19, 2013 ICD-9-CM Coordination and Maintenance Committee meeting is not yet available. This is expected to be posted on the CMS webpage in October, at:
and also on the CDC’s website page for the meetings.
Other Meeting materials (Agenda, Proposals and four YouTubes of the two-day September meeting proceedings) are now available from this page [3]:
There is an ICD-9-CM and ICD-10-CM/PCS revisions Timeline set out on pages 3 thru 7 of the Proposals PDF [2].
Submitting public comment:
The deadline for receipt of public and professional stakeholder comment on any of the proposed ICD-10-CM/PCS code revisions discussed at the September 18-19, 2013 ICD-9-CM Coordination and Maintenance Committee meeting is November 15, 2013.
Comments should be sent to the following NCHS email addresses:
Procedure comments by email to Pat Brooks, CMS: patricia.brooks2@cms.hss.gov
Diagnosis comments by email to Donna Pickett, CDC: nchsicd9CM@cdc.gov
Full contact details for submission of comments/objections to NCHS/CMS are on page 8 of the Proposals PDF. The meeting co-chairs state that electronic submissions are greatly preferred over snail mail in order to ensure timely receipt.
Responders are asked to consider the following:
Whether you agree with a proposal, disagree (and why), or have an alternative proposal to suggest.
But also to comment on the timing of those proposals that are being requested for approval for October 2014.
Does a proposal for a new or changed Index entry and Tabular List entry meet the criteria for implementation in Oct 2014 during a partial code freeze or should consideration for inclusion be deferred to Oct 2015 implementation? And separately, comment on the creation of a specific new code for the condition effective from October 1, 2015.
I shall post reminders before the November 15, 2013 deadline date and also a copy of the September meeting Summary document, once this is available. (Posting of the Summary document may be delayed due to the government shut-down and you may prefer to review the YouTubes of the meeting proceedings rather than wait for the Summary document to appear.)
References for key documents and screenshots:
1. Article: ICD Codes for Some DSM-5 Diagnoses Updated, Mark Moran, Psychiatric News, October 07, 2013:
http://psychnews.psychiatryonline.org/newsarticle.aspx?articleID=1757346
2. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting September 18-19, 2013:
http://www.cdc.gov/nchs/icd/icd9cm_maintenance.htm
September meeting Proposals document [PDF – 342 KB]:
http://www.cdc.gov/nchs/data/icd9/icd9cm_proposals_91819.pdf
3. ICD-9-CM/PCS Coordination and Maintenance Committee Meeting Sept 18-19, 2013 meeting materials and four YouTubes of proceedings:
http://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/ICD-9-CM-C-and-M-Meeting-Materials-Items/2013-09-18-MeetingMaterials.html
4. YouTube Videos from September 18, 2013 Meeting Day One
ICD-9-CM Coordination and Maintenance Committee Meeting (Morning Session) Part 1
http://www.youtube.com/watch?v=Ut3DmV88Dmc
ICD-9-CM Coordination and Maintenance Committee Meeting (Morning Session) Part 2
http://www.youtube.com/watch?v=CAE190sM5AQ
ICD-9-CM Coordination and Maintenance Committee Meeting (Afternoon Session) Part 3
http://www.youtube.com/watch?v=QQOFadq2x6U
September 19, 2013 Meeting Day Two
ICD-9-CM Coordination and Maintenance Committee Meeting Part 4
http://www.youtube.com/watch?v=G-pYdKyr_NE
5. Pages 45-46, Diagnosis Agenda:
 On 12 February, 24 year old Karina Hansen of Holstebro, Denmark, was removed from her home by five policemen, two doctors, two social workers and a locksmith, who threatened to break down the door to the family home.
On 12 February, 24 year old Karina Hansen of Holstebro, Denmark, was removed from her home by five policemen, two doctors, two social workers and a locksmith, who threatened to break down the door to the family home.
 2013 All rights reserved. Current Biology,
2013 All rights reserved. Current Biology, 

{kind=link}
Videos and meeting materials: September 18–19 ICD-9-CM Coordination and Maintenance Committee meeting
October 10, 2013 by admindxrw
Post #277 Shortlink: http://wp.me/pKrrB-3tV
This report relates to proposals submitted via the September ICD-9-CM/PCS Coordination and Maintenance Committee meeting for the inclusion of additional codes to the forthcoming US specific ICD-10-CM.
The twice yearly ICD-9-CM Coordination and Maintenance Committee meetings provide a public forum to discuss proposed code changes to ICD-9-CM and the ICD-10-CM/PCS. Next year, the committee, which is co-chaired by CMS and CDC, will be renamed to the ICD-10-CM Coordination and Maintenance Committee.
ICD-10-CM/PCS is scheduled for implementation in October 2014 and currently subject to partial code freeze.
The meeting scheduled on September 18, 2013 was devoted to both diagnosis and procedure code topics. The second day of the meeting, September 19, continued discussions related to diagnosis code topics.
Below are links for key meeting materials, four videocasts, and agenda item listings for the diagnosis proposals presented on Day Two (videocast Part 4). This includes the presentation of proposals by American Psychiatric Association (APA) Director of Research, Darrel Regier, MD, for insertion of new DSM-5 diagnoses into the ICD-10-CM.
Meeting materials:
+++
Videocasts for September 18, 2013 | Day One
Pat Brooks (CMS) Co-Chairperson
9:00 AM – 12:30 PM ICD-10-PCS Procedure presentations with public comment
12:30 PM – 1:30 PM Lunch break
1:30 PM – 5:00 PM Diagnosis presentations with public comment
Part 1 1:43 hours duration
Procedure presentations with public comment
+++
Part 2 1:27 hours duration
Procedure presentations with public comment
+++
Part 3 59 minutes duration
Diagnosis presentations with public comment
+++
Videocast for September 19, 2013 | Day Two
Donna Pickett (CDC) Co-Chairperson
+++
Part 4 1:42 hours duration
Diagnosis presentations with public comment
+++
Diagnosis proposals
Dr Regier concludes his presentation and hands podium back to Donna Pickett (CDC).
Donna Picket moves on to next set of proposals and turns podium over to Beth Fisher (CDC).
This concluded the diagnosis portion of the presentations.
Note that Agenda items from Page 53 onwards were tabled for presentation and discussion in earlier in the meeting proceedings.
Submitting public comment:
The deadline for receipt of public and professional stakeholder comment on any of the proposed ICD-10-CM/PCS code revisions discussed at the September 18-19, 2013 ICD-9-CM Coordination and Maintenance Committee meeting is November 15.
Comments should be sent to the following dedicated NCHS/CMS email addresses:
(Full contact details for submission of written comments/objections to NCHS/CMS on Page 8 of the Proposals/Diagnosis Agenda PDF. Electronic submissions are much preferred in order to ensure timely receipt.)
Share this:
Filed under American Psychiatric Association (APA), CDC, CMS, Criticism of DSM-V, DSM-5, DSM-5, ICD-10-CM, ICD-10-PCS, ICD-11, Somatic Symptom Disorder, WHO (World Health Organization) Tagged with american psychiatric association, binge eating disorder, disruptive mood dysregulation disorder, dsm-5, icd-10-cm, institute of psychiatry, NCHS, premenstrual dysphoric disorder, public comment, somatic symptom disorder